anaplastic meningioma

Anaplastic meningiomas (also known as malignant meningiomas) are uncommon, accounting for only ~1% of all meningiomas . Along with rhabdoid meningioma and papillary meningioma are considered WHO grade III tumors and demonstrate aggressive local growth and high recurrence rate.
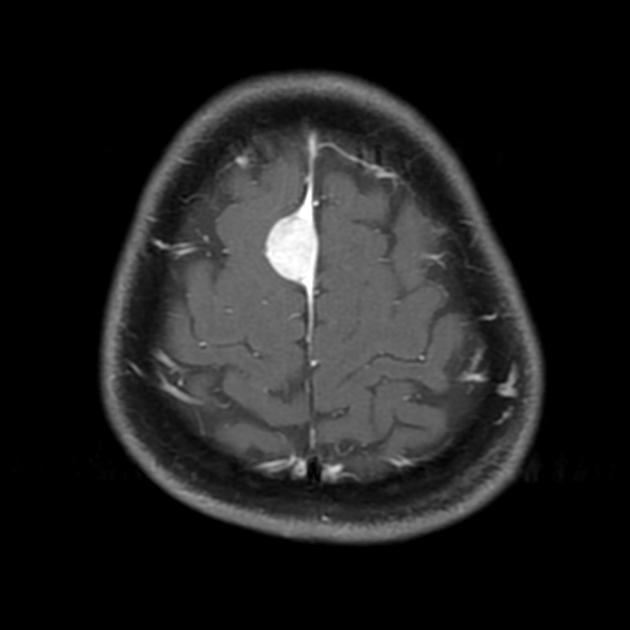
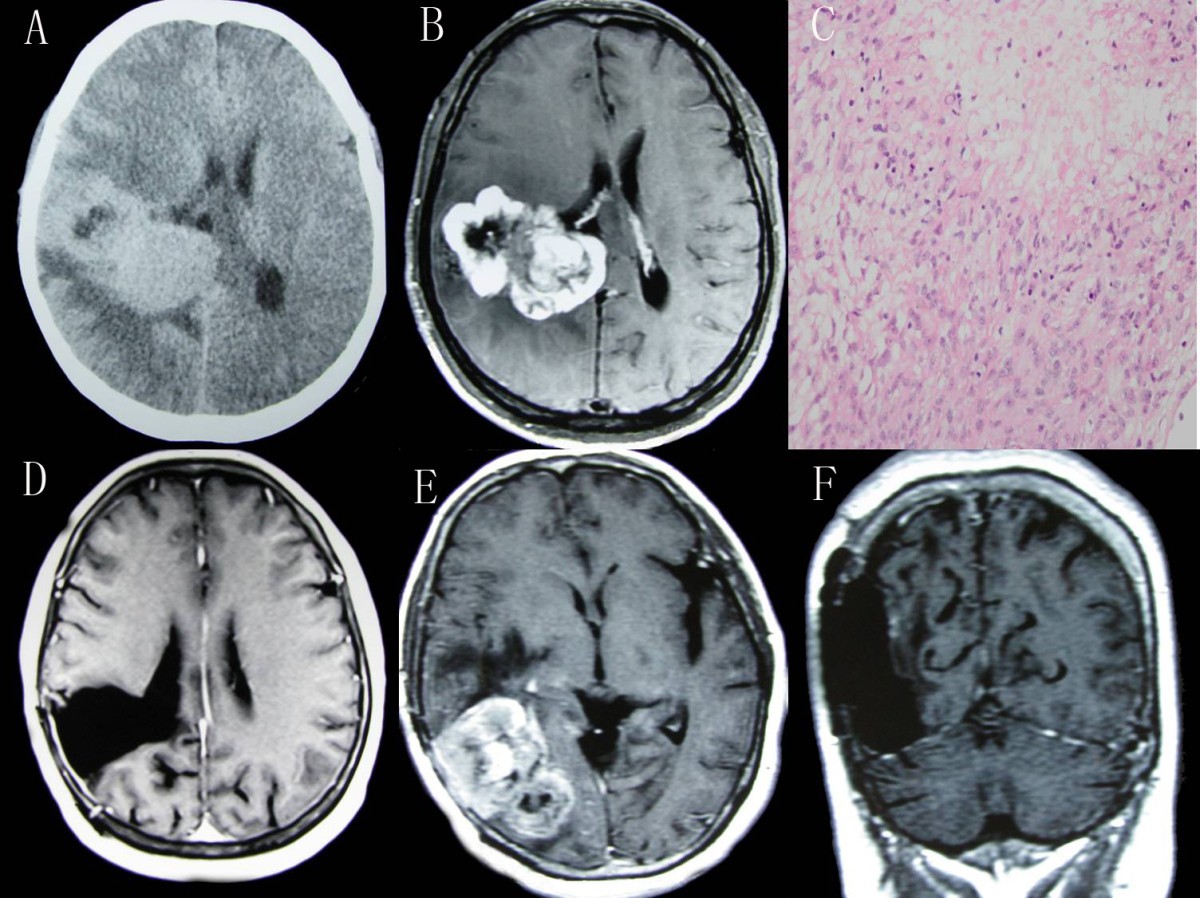
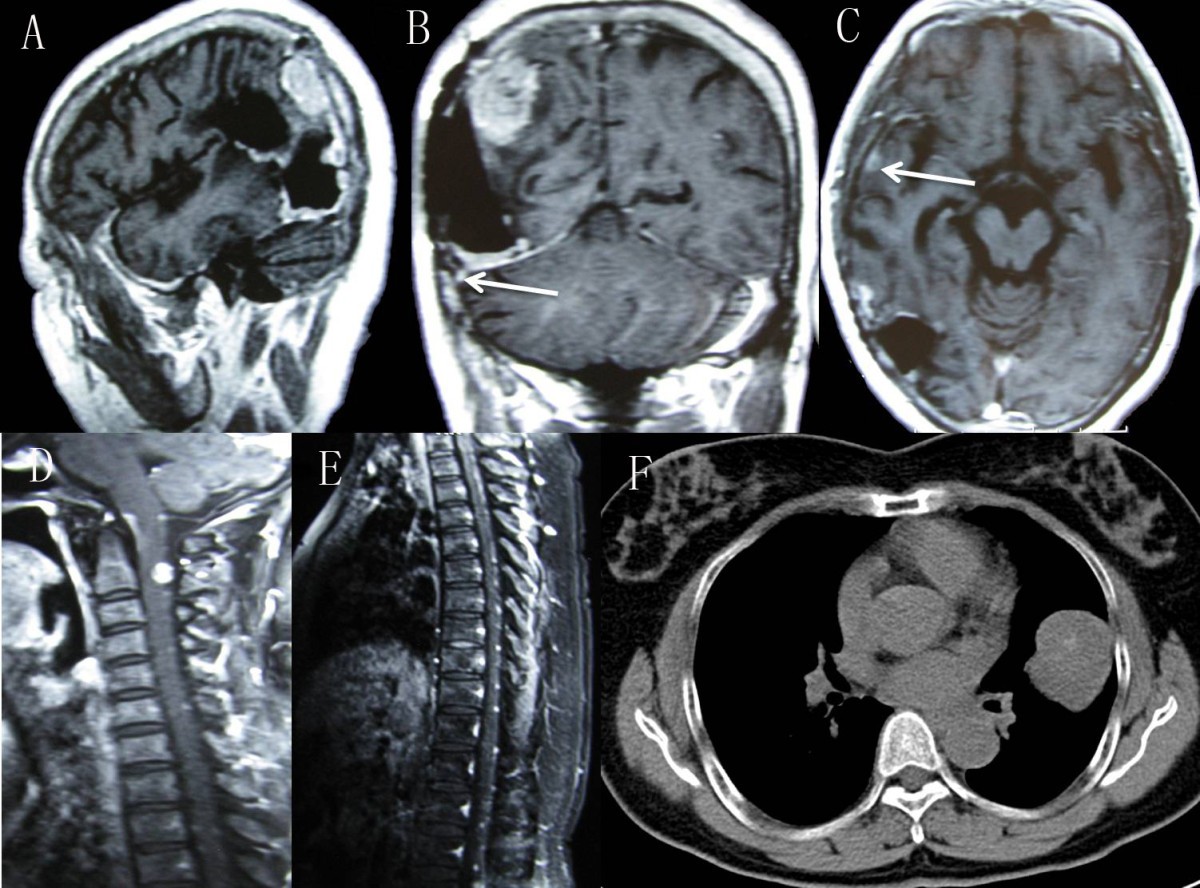
It should be noted that epidemiology, clinical presentation and radiographic features do not reliably distinguish anaplastic meningiomas from benign meningiomas (WHO grade I) and atypical meningiomas (WHO grade II), and thus that content is unnecessarily repeated here. Generally, these tumors grow faster, have more heterogeneous/aggressive imaging appearances, and have a tendency to recur early.
Pathology
Anaplastic meningiomas are those with the following histological characteristics :
- obvious malignant features similar to those seen in melanoma, carcinoma, or high-grade sarcoma
- 20 or more mitosis per ten high-power fields
Radiographic features
Generally, it is not possible to confidently distinguish benign (WHO grade I) and atypical (WHO grade II) from anaplastic (WHO grade III) meningiomas on general morphology. The most reliable feature in suggesting a non-grade I tumor is the presence of lower ADC values (reflecting higher cellularity) .
Importantly presence of vasogenic edema in adjacent brain parenchyma is not a predictor of atypical or anaplastic histology .
Brain invasion, although by definition denoting at least a grade II tumor, is also surprisingly difficult to predict on MRI.
Treatment and prognosis
First line therapy is surgical resection with radiotherapy (external beam or brachytherapy) often added both for complete and incomplete resections (see Simpson grade). Radiation has been shown to improve local control and prolongs overall survival .
No effective chemotherapeutic agents have been identified .
The recurrence rate is significantly higher (50-94%) than that seen in grade II meningiomas (29-52%) and this correlates with reduced survival .
Siehe auch:


 Assoziationen und Differentialdiagnosen zu malignes Meningeom:
Assoziationen und Differentialdiagnosen zu malignes Meningeom: