centrilobular pulmonary emphysema


Centrilobular pulmonary emphysema is the most common morphological subtype of pulmonary emphysema.
Epidemiology
It may be found in up to one-half of adult smokers at autopsy .
Risk factors
- cigarette smoking
Pathology
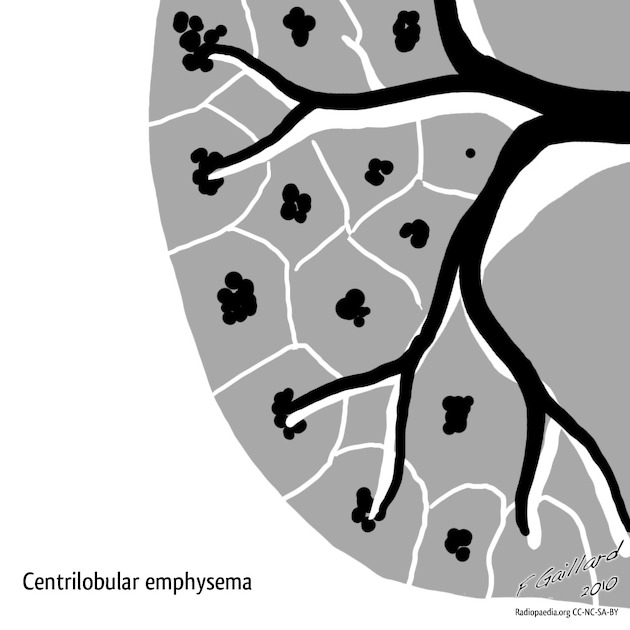
The pathological process of centrilobular emphysema typically begins near the center of the secondary pulmonary lobule in the region of the proximal respiratory bronchiole. Selective lung destruction results in the characteristic apposition of the normal and emphysematous lung. The resulting area of destruction surrounded by normal tissue allows appreciation of key structural lesion evident to the naked eye ”emphysematous space".
Location
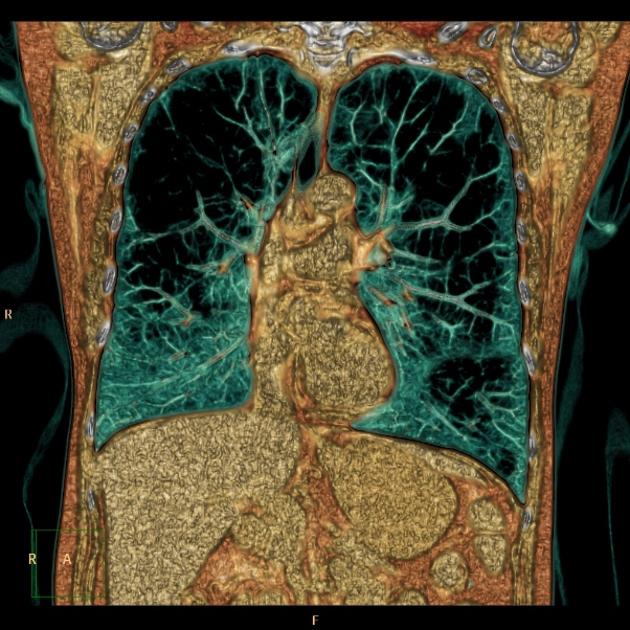
- there is usually an upper lobe predilection
Classification
One method of sub-classification according severity is as
- trace centrilobular emphysema
- mild centrilobular emphysema
- moderate centrilobular emphysema
- confluent centrilobular emphysema
- coalescent centrilobular or lobular lucencies with multiple regions spanning several secondary pulmonary lobules but not involving hyperexpansion of secondary pulmonary lobules and distortion of pulmonary architecture
- advanced destructive emphysema (ADE)
- panlobular radiolucencies with hyperexpansion of secondary pulmonary lobules and distortion of pulmonary architecture
Radiographic features
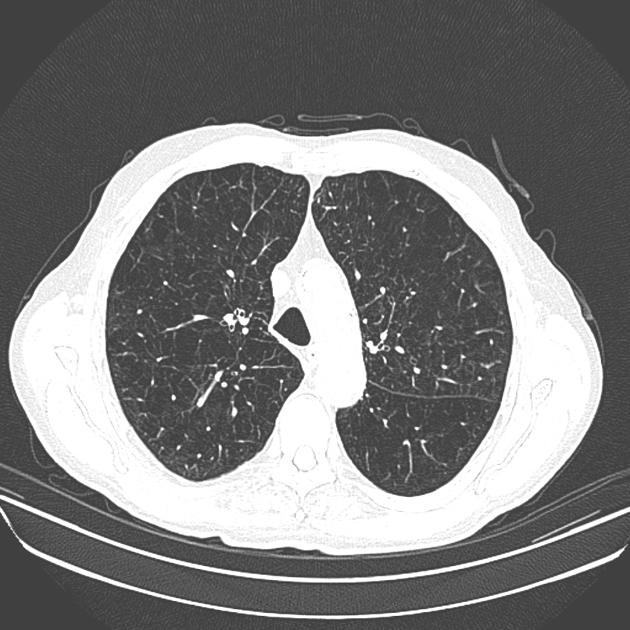
CT
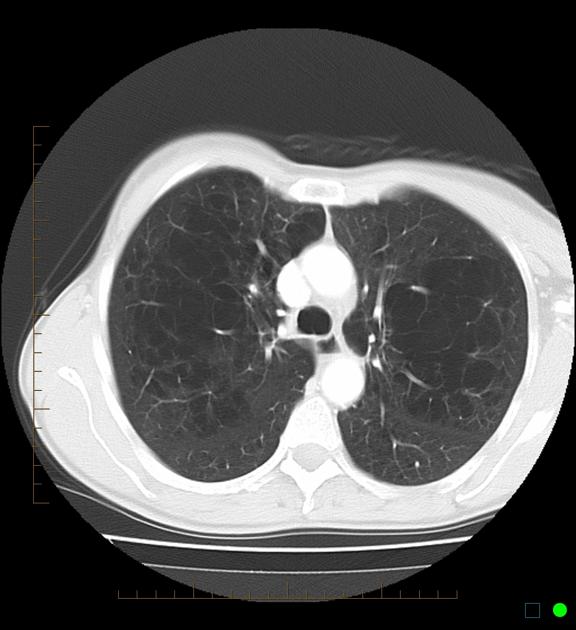
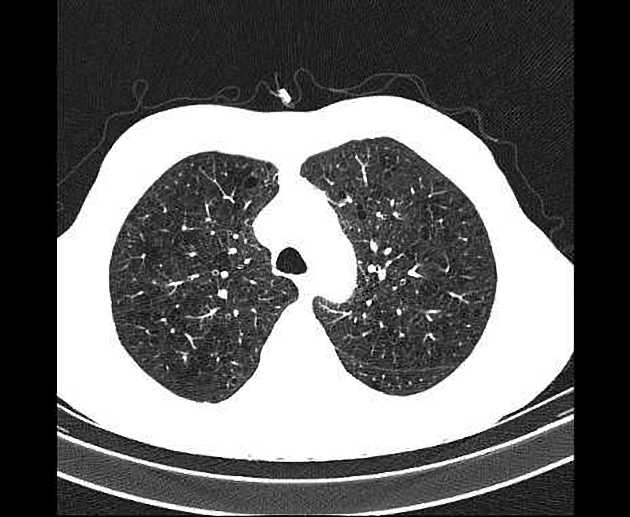
Early changes
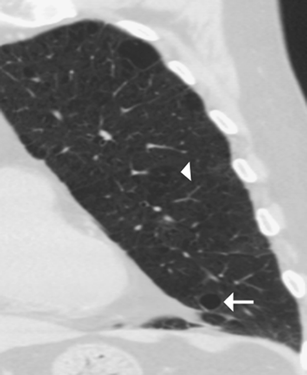
Early centrilobular emphysema is usually seen as small round black (low attenuating) evenly distributed holes with ill-defined borders that may appear in the central portion of the secondary pulmonary nodule around the centrilobular artery.
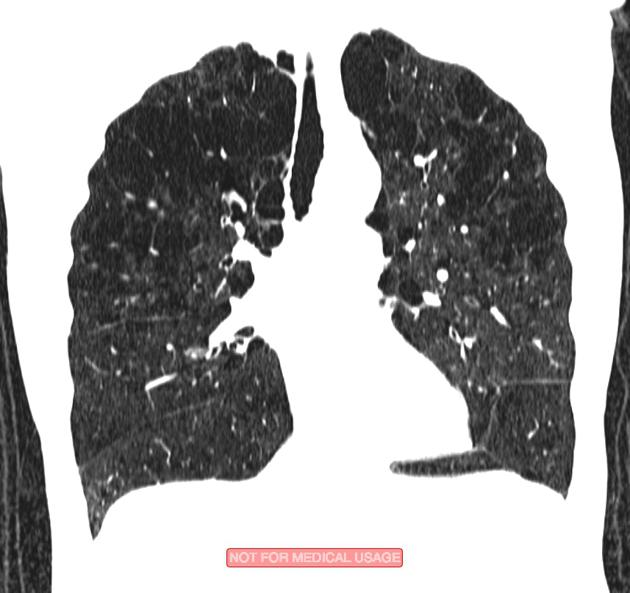
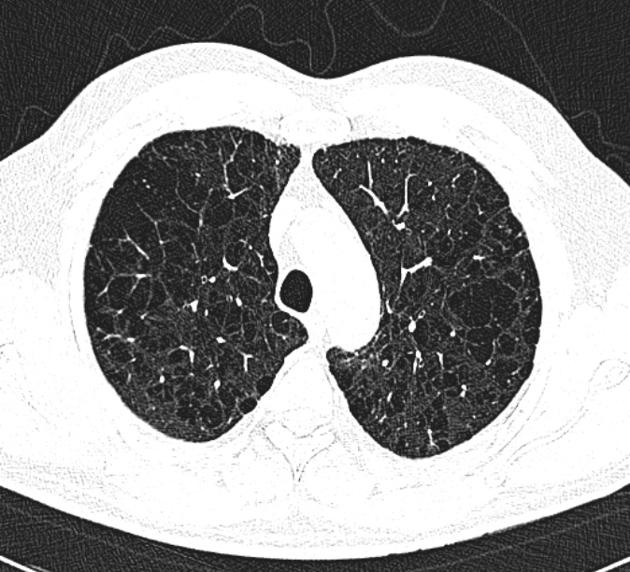
Late changes
As the emphysematous process progresses, the low-attenuation areas become confluent and inseparable.
With the enlargement of the dilated airspace, the surrounding lung parenchyma is compressed, which enables observation of a clear border between the emphysematous area and the normal lung. Since the disease progresses from the centrilobular portion, normal lung parenchyma in the perilobular portion tends to be preserved .
The pulmonary vessels in areas of severe emphysema are small, with shunting of blood flow to lung parenchyma that can better exchange air to maintain matched ventilation and perfusion.
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu zentrilobuläres Emphysem:
Assoziationen und Differentialdiagnosen zu zentrilobuläres Emphysem: