colloid cyst of the third ventricle








Colloid cysts of the third ventricle are benign epithelial lined cysts with characteristic imaging features. Although usually asymptomatic, they can rarely present with acute and profound hydrocephalus.
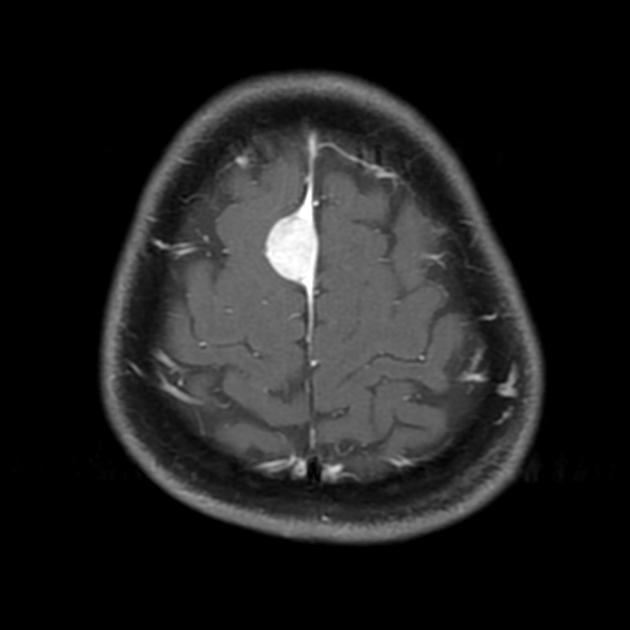
Classically these cysts are identified as a well-delineated hyperattenuated mass on unenhanced CT, attached to the anterosuperior portion of the third ventricle. On MRI they usually are hyperintense on T1 and isointense to brain on T2 weighted images. Peripheral rim enhancement may be present in some cases.
Epidemiology
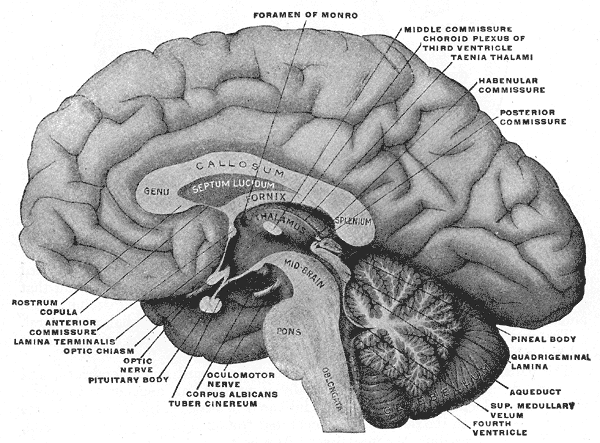
Colloid cysts account for ~2% (range 0.5-3%) of primary brain tumors and 15-20% of intraventricular masses . They are located at the foramen of Monro in 99% of cases .
The majority of cases are identified in early middle age (30-40 years of age) although 8% of cases may be diagnosed in pediatric age .
Clinical presentation
In the vast majority of cases, colloid cysts are found incidentally and are asymptomatic. Their position in the roof of the third ventricle immediately adjacent to the foramina of Monro can on occasion result in sudden obstructive hydrocephalus and can present with a thunderclap headache or unconscious collapse. The headaches tend to be positional, and patients may learn how to relieve symptoms.
Pathology
Colloid cysts originate from the abnormal folding of the primitive neuroepithelium (the paraphysis elements) . They contain mucin, old blood (hemosiderin), cholesterol, and various ions, accounting for a wide range of imaging appearance.
These cysts are lined by a single layer of columnar epithelium which produces mucin, which appears as a thick yellow-green fluid when the cyst is open.
Radiographic features
Cross-sectional imaging usually enables the diagnosis to be made with confidence. MRI is superior to CT in fully characterizing the lesion.
On all modalities, colloid cysts appear as a rounded, sharply demarcated lesion at the foramen of Monro, which range in size from a few millimeters to 3-4 cm .
CT
Typically seen as a well-defined, rounded lesion at the roof of the 3ventricle:
- unilocular
- typically hyperdense
- isodense and hypodense cysts are uncommon
- calcification is uncommon
MRI
MR signal characteristics include:
- T1: variable
- ~50% high signal
- the rest are hypointense or isointense to adjacent brain
- T1 C+ (Gd): only rarely demonstrates thin rim enhancement, but usually this represents an enhancement of the adjacent and stretched septal veins
- T2: variable
- most are of low T2/T2* signal (short T2), related to thick "motor oil" consistency fluid
- some have central low T2 and high peripheral T2 signal
- some are homogeneously high signal
- FLAIR: cysts which are of low signal on T2 will appear similar to attenuated CSF on FLAIR, and are thus difficult to appreciate
Treatment and prognosis
They tend to gradually increase in size over time and if resection is required, this can be performed via a transcallosal approach or more recently endoscopically or stereotactically.
When large and or symptomatic the decision to operate is relatively straightforward, as it can be life-saving. For small lesions without symptoms attributable to them, the careful discussion between the patient and treating surgeon is required to weigh up the pros and cons of surgical intervention.
The options are open or endoscopic resection or endoscopic or stereotactic aspiration. Aspiration may fail if the content of the cyst is too viscous, which can be predicted by appreciating low signal on T2 weighted sequences .
Differential diagnosis
There are usually no differential diagnoses for a colloid cyst. In atypical cases, it is worth considering other masses which arise in the region of the foramen of Monro, including:
- calcified or hyperdense meningioma
- giant cell astrocytoma
- pilocytic astrocytoma
- blood in the region of the foramen of Monro
For a more complete list please refer to masses in the region of the foramen of Monro.
Practical points
- size of cyst
- T2 signal intensity of the cyst (low signal = difficult to aspirate )
- size of ventricles
- presence of cavum septum pellucidum et vergae
- presence and location of internal cerebral veins
- presence of any abnormal vascular structures (e.g. DVA) that may be present along the surgical tract
Siehe auch:
- Meningeom
- Pilozytisches Astrozytom
- intraventrikuläre Neoplasien und Läsionen
- interventricular foramen (of Monro)
- intraventrikuläre Kolloidzyste
- Verschlusshydrocephalus
- Kolloidzyste
- intraventrikuläre Neoplasien und Läsionen - Überblick
- Riesenzellastrozytom
- Cerebralshunt
- masses in the region of the foramen of Monro
und weiter:


 Assoziationen und Differentialdiagnosen zu Kolloidzyste des dritten Ventrikels:
Assoziationen und Differentialdiagnosen zu Kolloidzyste des dritten Ventrikels: