Desmoid-Tumor - aggressive Fibromatose







Aggressive fibromatosis is a type of musculoskeletal fibromatosis. While it is a non-metastasizing fibrous lesion, it is thought to be a true neoplasm that arises from the fascial and musculoaponeurotic coverings, sometimes at the site of a traumatic or post-surgical scar.
Terminology
The term aggressive fibromatosis is occasionally used synonymously with desmoid tumors by some authors . This article will focus in the musculoskeletal presentation of this tumor; for the abdominal presentation, please refer to the latter.
Epidemiology
According to one the study, the mean age at presentation is ~40 . There may be a slight female predilection (male to female ratio of 1:1.2).
Pathology
Being non-encapsulated, poorly circumscribed, and infiltrative, aggressive fibromatosis grows insidiously and invades locally. The lesions may become quite large and adhere to neighboring structures, such as neurovascular bundles. The lesions grossly resemble scar tissue and are composed of well-differentiated fibroblasts embedded in an abundant collagenous matrix with increased cellularity at the periphery. Cytologic features of malignancy are lacking. Its exact cause is unknown.
Associations
Recognized associations include:
- surgical or accidental trauma
- pregnancy
- oestrogenic hormone use
- Gardner syndrome
- familial adenomatous polyposis
Location
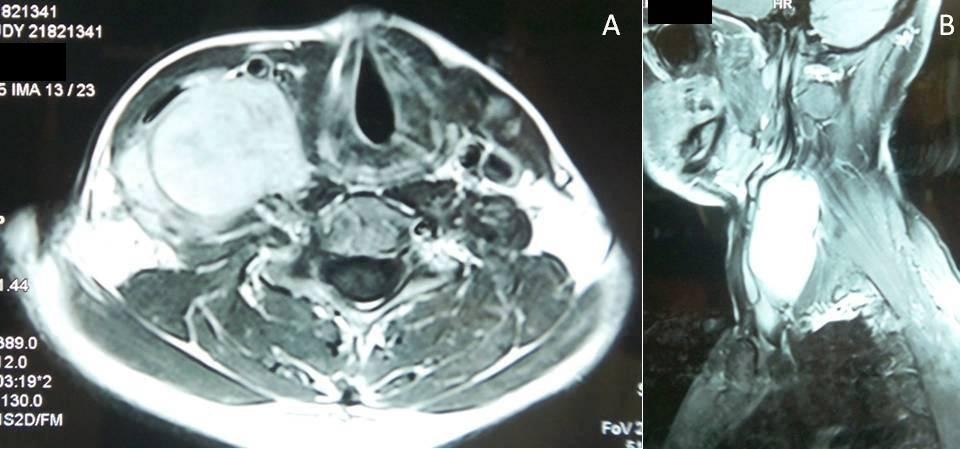
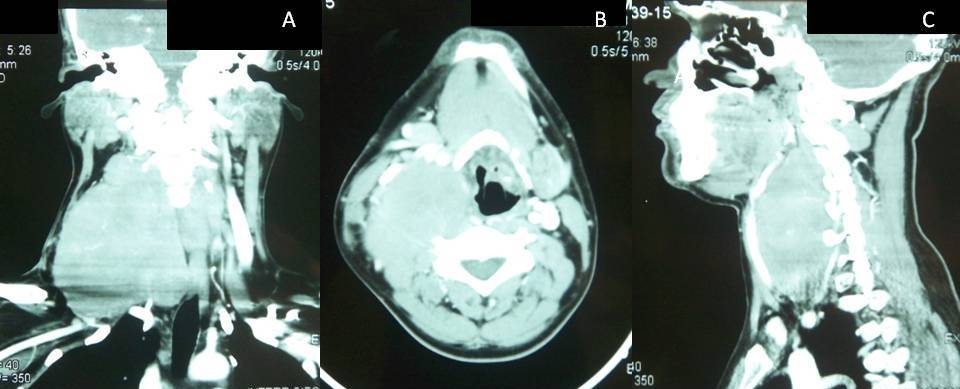
Aggressive fibromatosis can occur in the superficial or deep soft tissues anywhere in the body. However, the head and neck regions have been reported in 25% of cases, with the supraclavicular fossae and neck being the most common locations.
Classification
Desmoid-type fibromatosis is listed in the WHO classification of soft tissue tumors under the category "fibroblastic/myofibroblastic tumors."
Radiographic features
They tend to be poorly marginated infiltrating the surrounding tissues, the lack of metastasis can help distinguish aggressive fibromatosis from a fibrosarcoma.
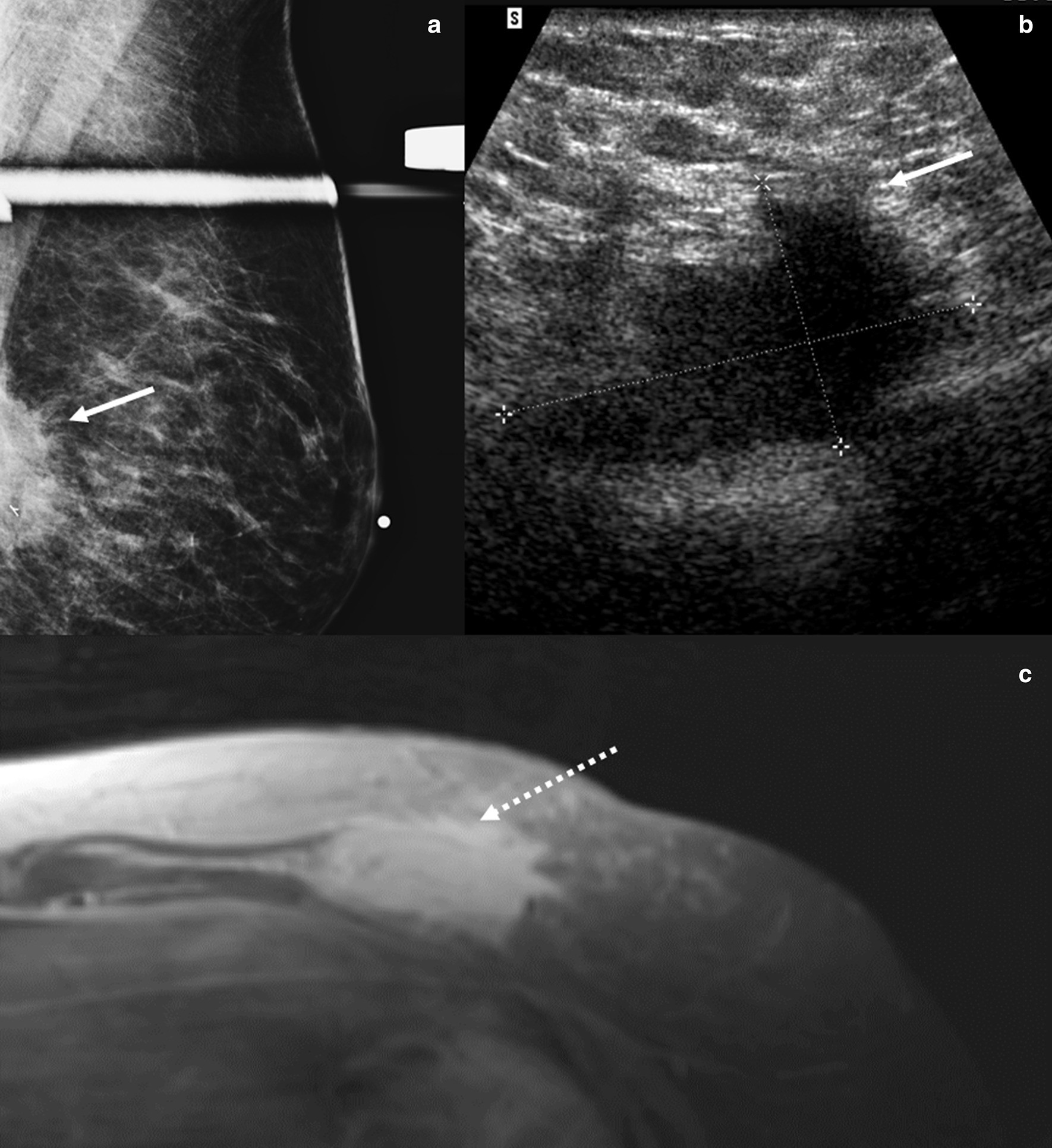
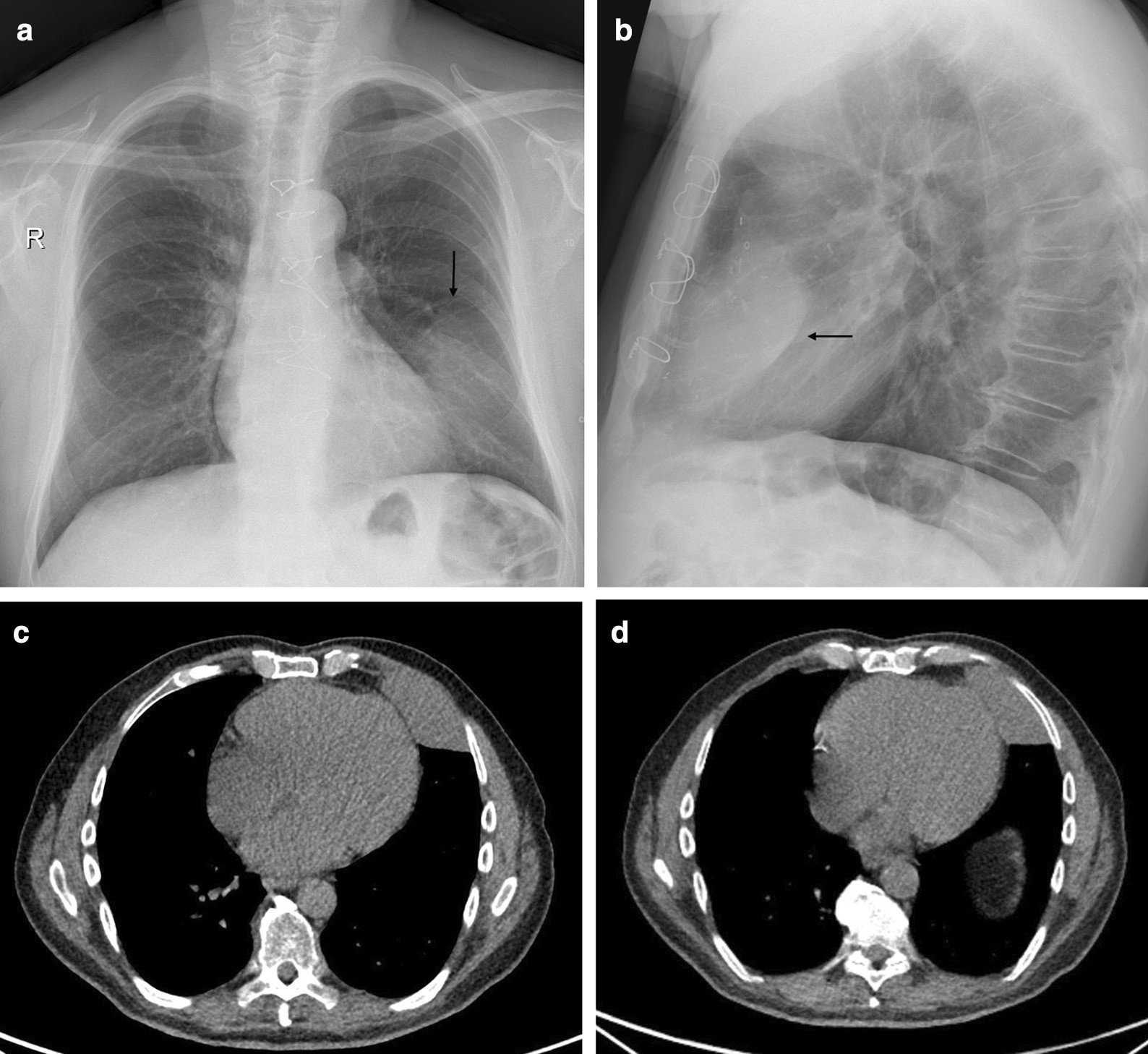
Plain radiograph
Radiographs may show a soft-tissue mass, localized periosteal thickening, or direct bony destruction/invasion .
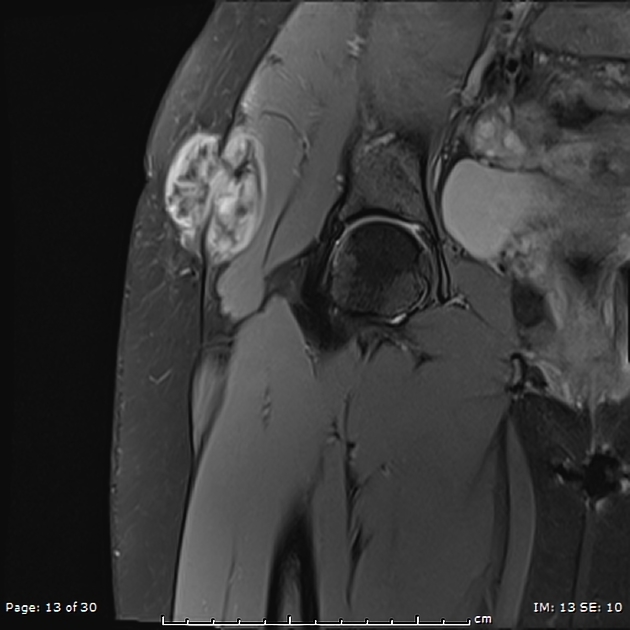
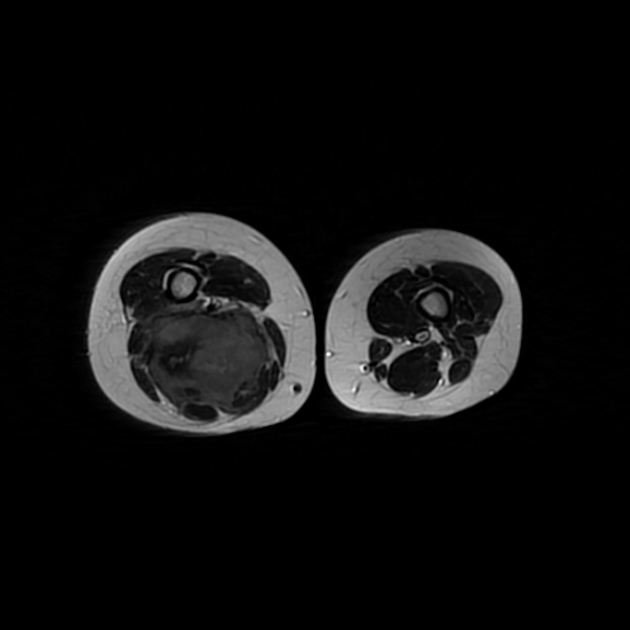
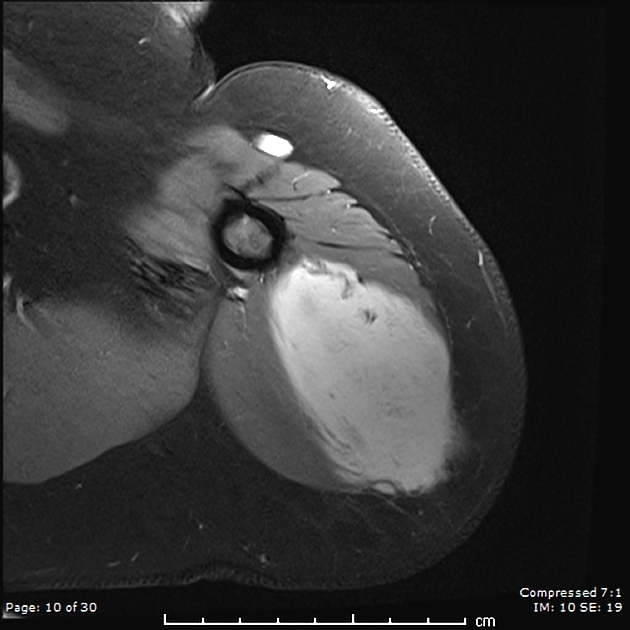
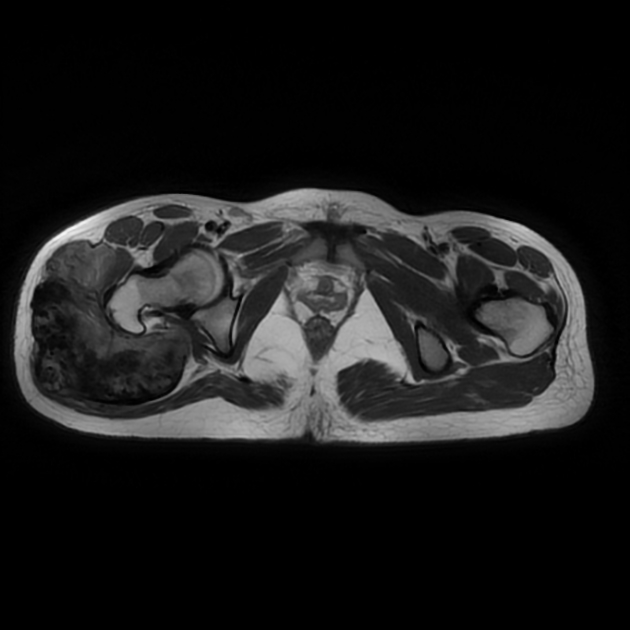
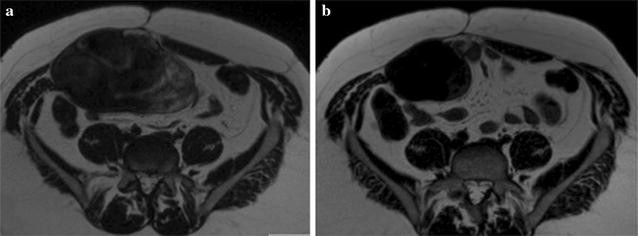
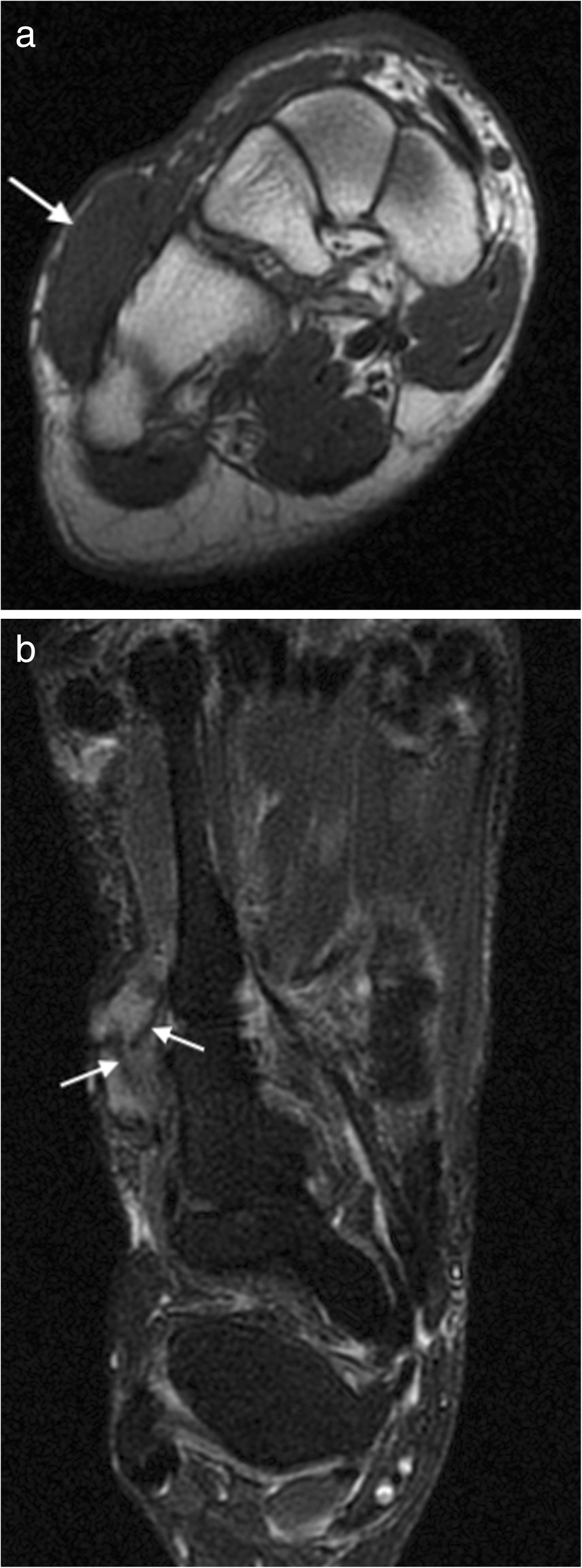
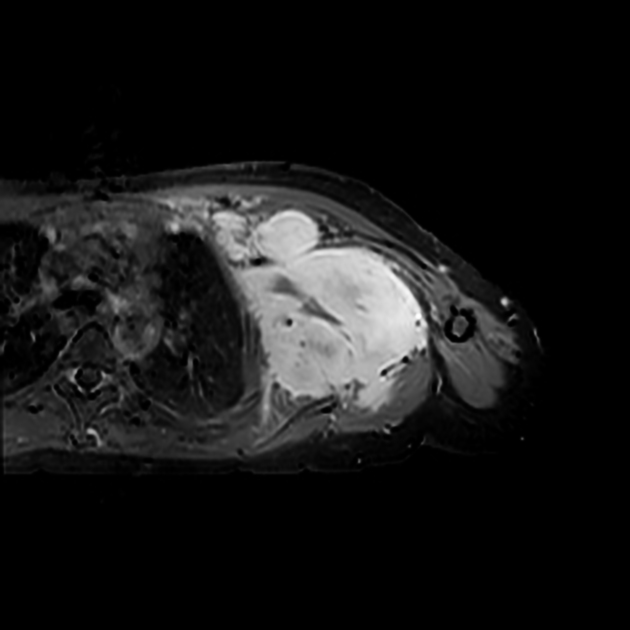
MRI
Signal characteristics of the lesion include :
- T1: homogeneously isointense or mildly hyperintense
- T2/STIR: high heterogeneous signal
- T1 C+ (Gd): typically enhances avidly
- GE: peripheral areas of smooth low signal intensity that do not represent calcification (check radiographs) or hemorrhage (check gradient images/scouts for blooming) are characteristic
Angiography
May show arterial stretching, neovascularity, and tumor staining .
Treatment and prognosis
It does not have any propensity for metastasis although it can aggressively invade structures. The optimal management for aggressive fibromatosis depends on tumor location and extent. Surgical resection may be offered although the likelihood of local recurrence after surgery is high, particularly if margins are positive. Moderate-dose radiotherapy alone for gross disease or after a microscopically incomplete resection yields local control rates of approximately 75-80% . Treatment with pharmacologic agents results in objective response rates of approximately 40-50%.
Differential diagnosis
- fibrosarcoma
- aggressive osseous tumors
- aggressive schwannoma
See also
Siehe auch:
- Gardner-Syndrom
- mesenteriale Fibromatose
- Desmoid-Tumor der Bauchwand
- desmoplastisches Fibrom
- WHO Klassifikation der Weichteiltumoren
- musculoskeletal fibromatoses
- intraabdominal desmoid tumor
und weiter:
- Läsionen der Rippen
- kortikales Desmoid
- Pleomorphes Undifferenziertes Sarkom
- Fibromatose der Mamma
- Fasciitis nodularis
- Infantile Myofibromatose
- permeative process in bone (mnemonic)
- Riesenzelltumor der Sehnenscheiden
- desmoid tumours complicating familial adenomatous polyposis
- Fibromatose Kniegelenk
- infantile desmoid-type fibromatosis
- retropharyngealer Desmoidtumor
- pleurale aggressive Fibromatose
- Desmoid-Tumor der Bauchwand bei Kindern


 Assoziationen und Differentialdiagnosen zu Desmoid-Tumor - aggressive Fibromatose:
Assoziationen und Differentialdiagnosen zu Desmoid-Tumor - aggressive Fibromatose:

