Ductus thyreoglossus Fistel
Ductus thyreoglossus Fistel
Ductus thyreoglossus Zyste Radiopaedia • CC-by-nc-sa 3.0 • de
Thyroglossal duct cysts (TGDC) are the most common type of congenital neck cysts and pediatric neck masses. They are typically located in the midline and are the most common midline neck mass in young patients. They can be diagnosed with multiple imaging modalities including ultrasound, CT and MRI.
Epidemiology
Thyroglossal duct cysts typically present during childhood (90% before the age of 10 years) as a gradually growing painless fluctuant cervical mass or remain asymptomatic until they become infected, in which case they can present at any time.
Thyroglossal duct cysts account for 70% of all congenital neck anomalies, and are the second most common benign neck mass after lymphadenopathy.
Associations
- ectopic thyroid: ~40%
Clinical presentation
The presentation is typically either as a painless rounded midline anterior neck swelling or if infected, as a red warm painful lump. It may move with swallowing and classically elevates on tongue protrusion.
Pathology
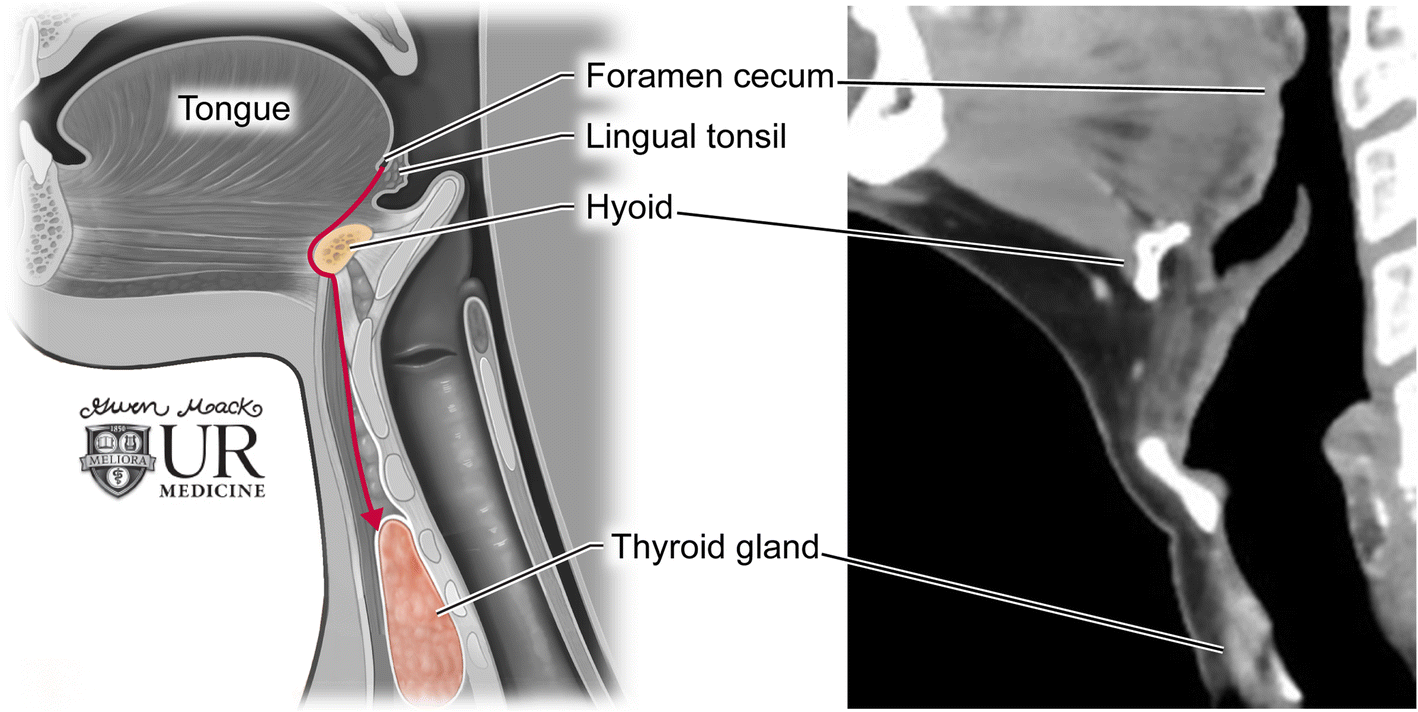
Thyroglossal duct cysts are epithelial-lined cysts. They result from failure of normal developmental obliteration of the thyroglossal duct during development (8 - 10 gestational week) and can thus occur anywhere along the course of the duct.
The epithelial lining of the cyst varies with location. Those that form near the tongue are lined by stratified squamous epithelium. The more common cysts located in the neck are lined with cells similar to thyroidal acinar epithelium.
Location
The cysts can occur anywhere along the course of the thyroglossal duct from the foramen cecum to the thyroid gland although infrahyoid location is most common:
- suprahyoid: 20-25% (less common in adults ~5%)
- at the level of hyoid bone: ~30% (range 15-50%)
- infrahyoid: ~45% (range 25-65%)
Typically, they are located in the midline (~70%) with those off-midline characteristically adjacent to the thyroid cartilage. Almost all thyroglossal duct cysts are located within 2 cm of the midline, with more inferior lesions tending to be off midline.
Radiographic features
Ultrasound
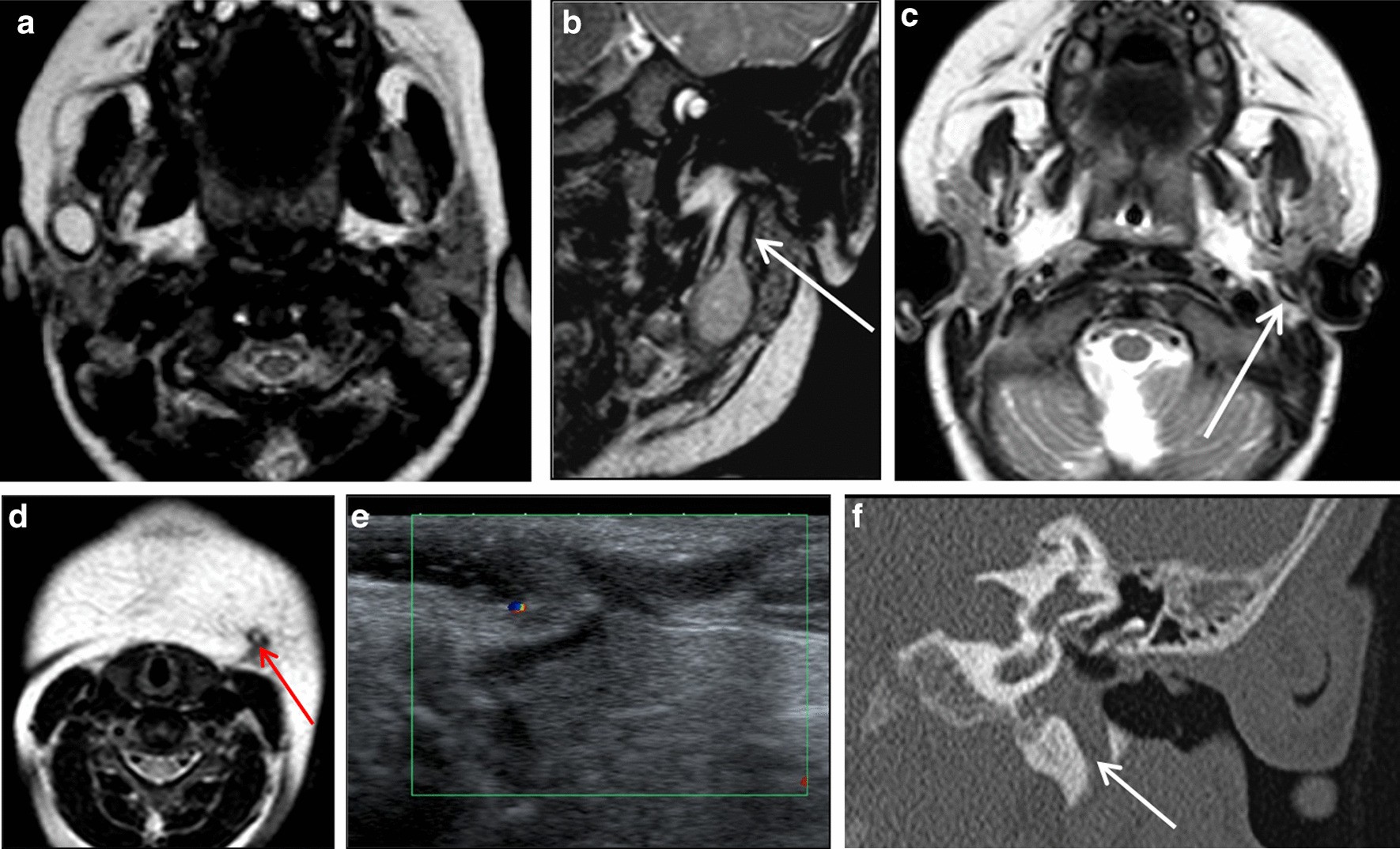
Unless infected, they are painless, fluctuant cystic structures which splay the strap muscles with posterior acoustic enhancement. The fluid is usually hypo- or anechoic and the walls are thin without internal vascularity.
However, in some cases, there may be internal complexity. The internal fluid may contain debris and septa or internal echoes from proteinaceous material. This is even in the absence of infection, particularly the case in an adult patient where cysts may be complex heterogeneous masses.
If there is associated infection, there may be thickened/irregular walls, increased blood flow and surrounding inflammatory change.
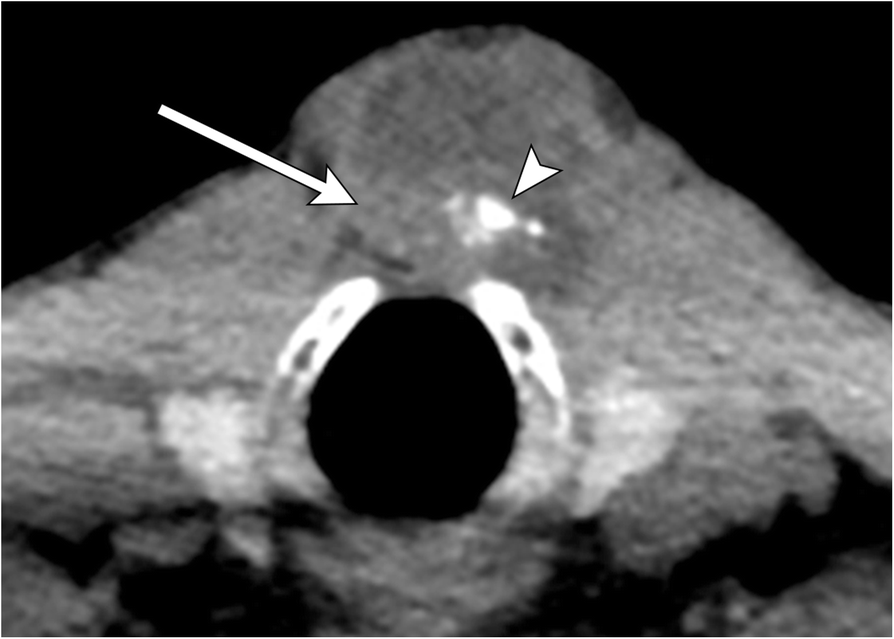
A soft tissue lesion in association with the cyst may be ectopic thyroid tissue or rarely represents carcinoma (usually papillary origin).
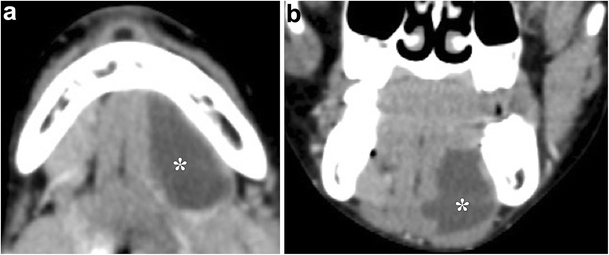
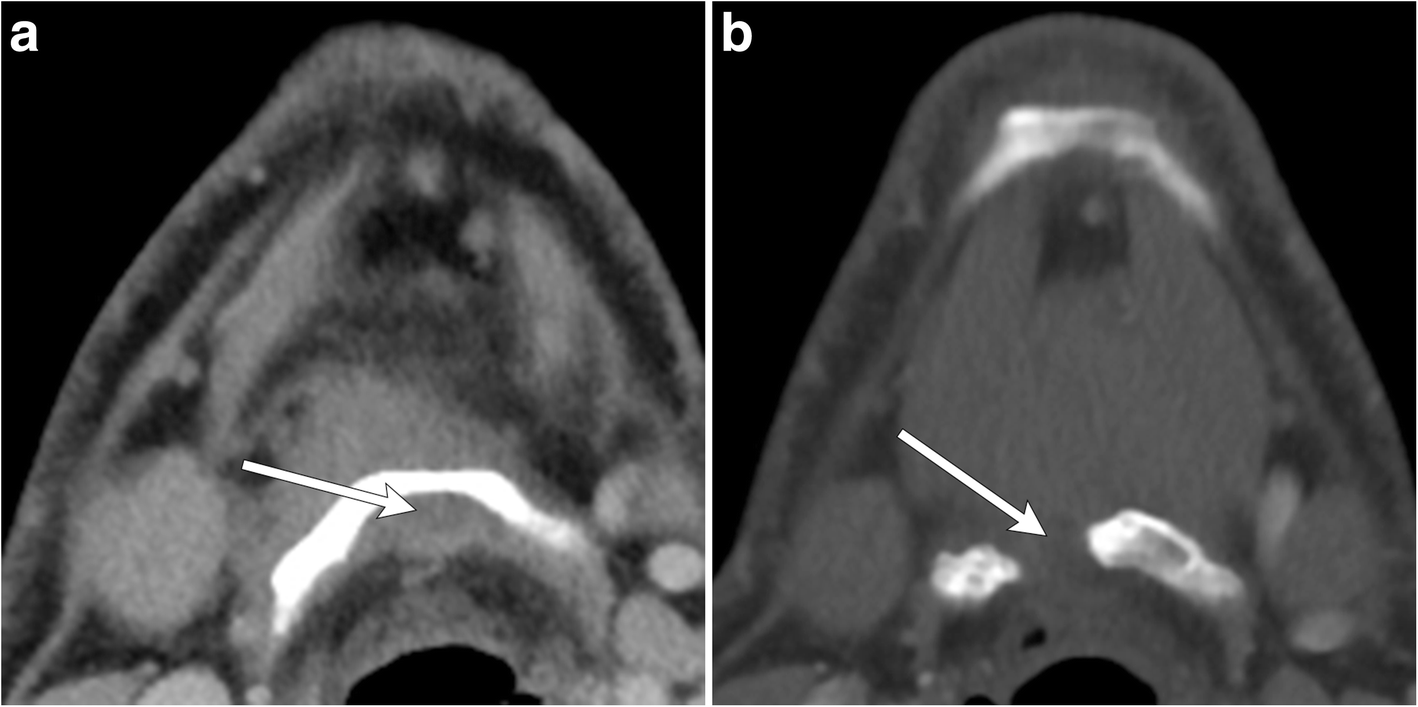
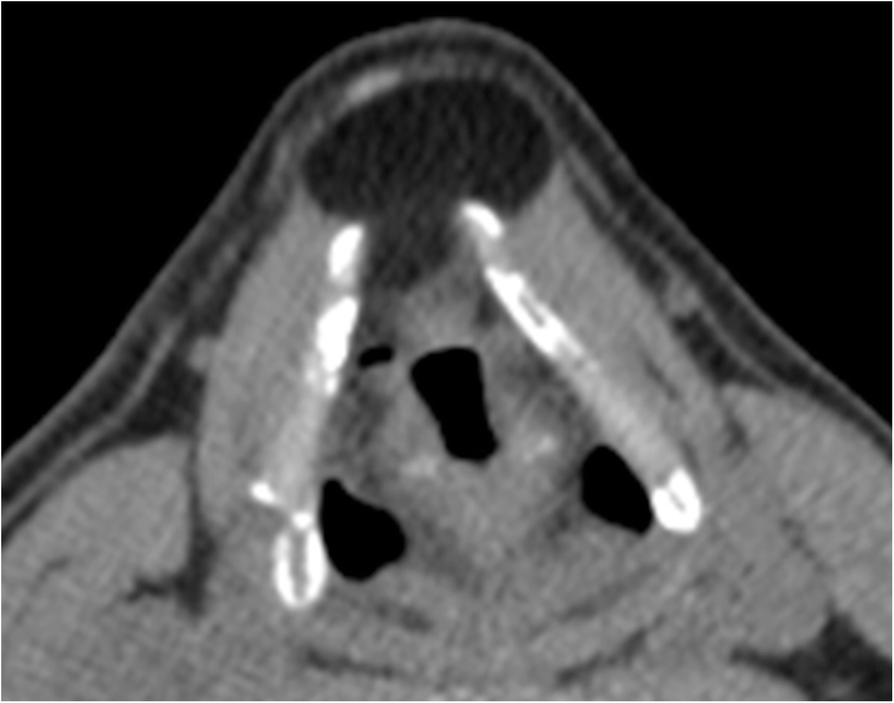
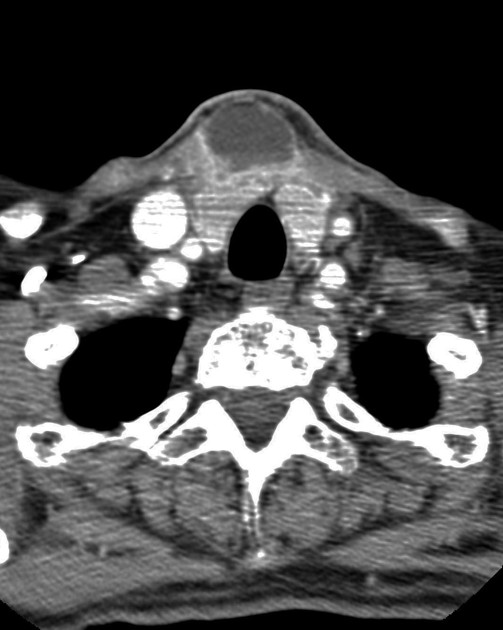
CT
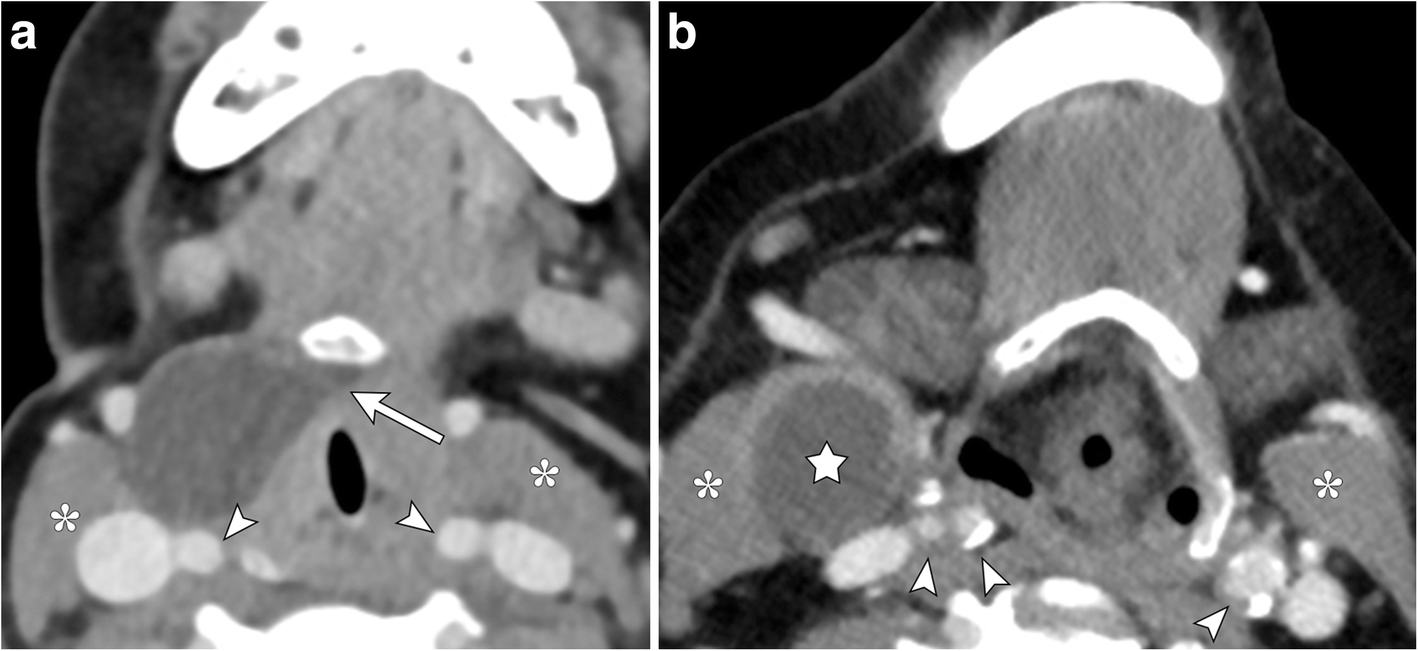
At CT, thyroglossal duct cysts are thin-walled, smooth, well-defined homogeneously fluid-density lesions with an anterior midline or paramedian location. The generally accepted rule is that they should be within 2 cm of the midline. They may demonstrate slight rim (capsular) enhancement.
The sternocleidomastoid muscle is typically displaced posteriorly or posterolaterally. In some cases, thyroglossal duct cysts may be embedded in the infrahyoid (strap) muscles.
MRI
- T1: variable
- low signal: if low protein or uncomplicated
- high signal (most common ) due to:
- previous hemorrhage or infection
- high protein (probably due to previous complication)
- T2: typically high signal
- T1 C+ (Gd)
- no enhancement in uncomplicated cysts
- thin peripheral enhancement may be seen
Treatment and prognosis
Complete resection of the cyst and duct up to the foramen cecum is curative. The Sistrunk procedure includes resection of the middle third of the hyoid bone. There is a small risk of recurrence (~2.5%).
Complications
- infection
- malignancies do occur but are rare
- seen in <1% of cysts
- when they do occur they are most frequently papillary thyroid carcinoma
- presence of calcification is suggestive of malignancy, while intracystic soft tissue is less specific
Differential diagnosis
The differential is that of midline neck masses:
- branchial cleft cyst: three times less common, and usually well away from the midline
- Delphian adenopathy
- epidermoid cyst: superficial to the strap muscles
- thyroid cyst or thyroid neoplasm
- laryngocele
- ranula
- parathyroid adenoma
- ectopic thyroid
Siehe auch:
- Laryngozele
- Lobus pyramidalis
- Ductus thyreoglossus
- Ductus thyreoglossus Zyste
- thyroid neoplasm
- Kiemenbogenzyste
- Ductus thyreoglossus Zyste mit Karzinom
- Mundbodenzyste (Ranula)
- zervikale Mittellinienraumforderungen
- Sistrunk-Resektion
- laryngeale Dermoidzyste
- Delphischer Lymphknoten
- kongenitale zervikale Mittellinienspalte
und weiter:


 Assoziationen und Differentialdiagnosen zu Ductus thyreoglossus Fistel:
Assoziationen und Differentialdiagnosen zu Ductus thyreoglossus Fistel: