extension supracondylar fractures















Supracondylar humeral fractures, often simply referred to as supracondylar fractures, are a classic pediatric injury which requires vigilance as imaging findings can be subtle.
Epidemiology
Simple supracondylar fractures are typically seen in younger children, and are uncommon in adults; 90% are seen in children younger than 10 years of age, with a peak age of 5-7 years . These fractures are more commonly seen in boys .
These injuries are almost always due to accidental trauma, such as falling from a moderate height (bed/monkey-bars) .
Rarely (<5%) supracondylar fractures are seen due to a fall onto the flexed elbow. They occur in older individuals and require different management and are discussed separately: see flexion supracondylar fracture .
Mechanism
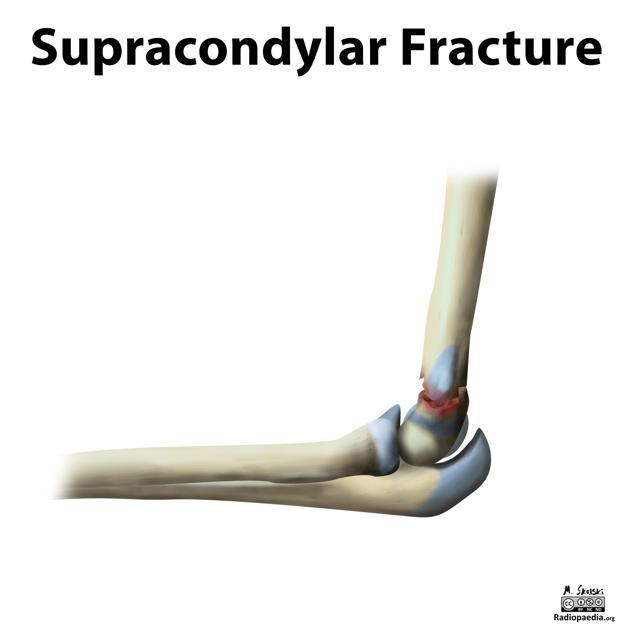
Typically supracondylar fractures occur as a result of a fall on a hyper-extended elbow. They result in an extra-articular fracture line, and (when displaced) posterior displacement of the distal component.
Radiographic features
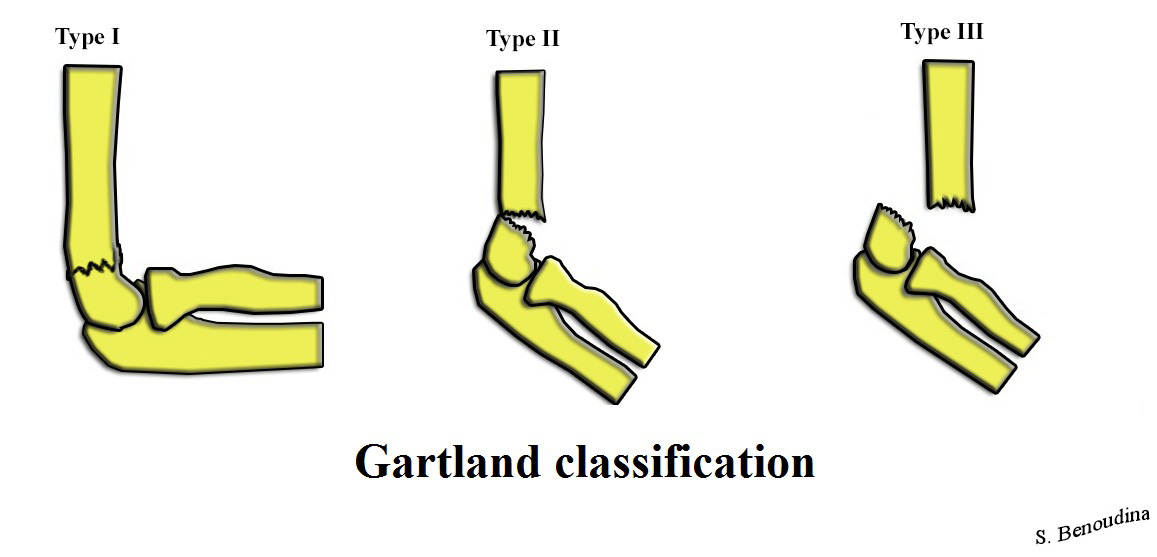
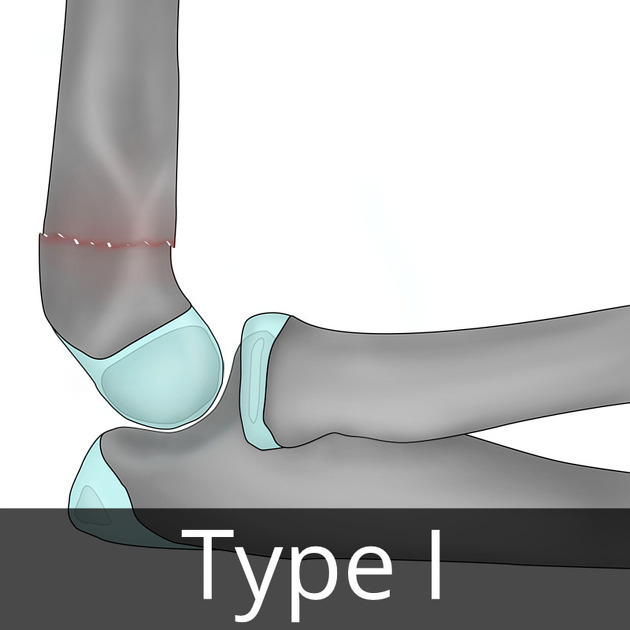
Classification of supracondylar fractures is relatively straightforward and based on three types :
- type I: undisplaced
- type II: displaced with intact posterior cortex
- type IIa: no rotational deformity
- type IIb: rotational deformity
- type III: complete displacement
Plain radiograph
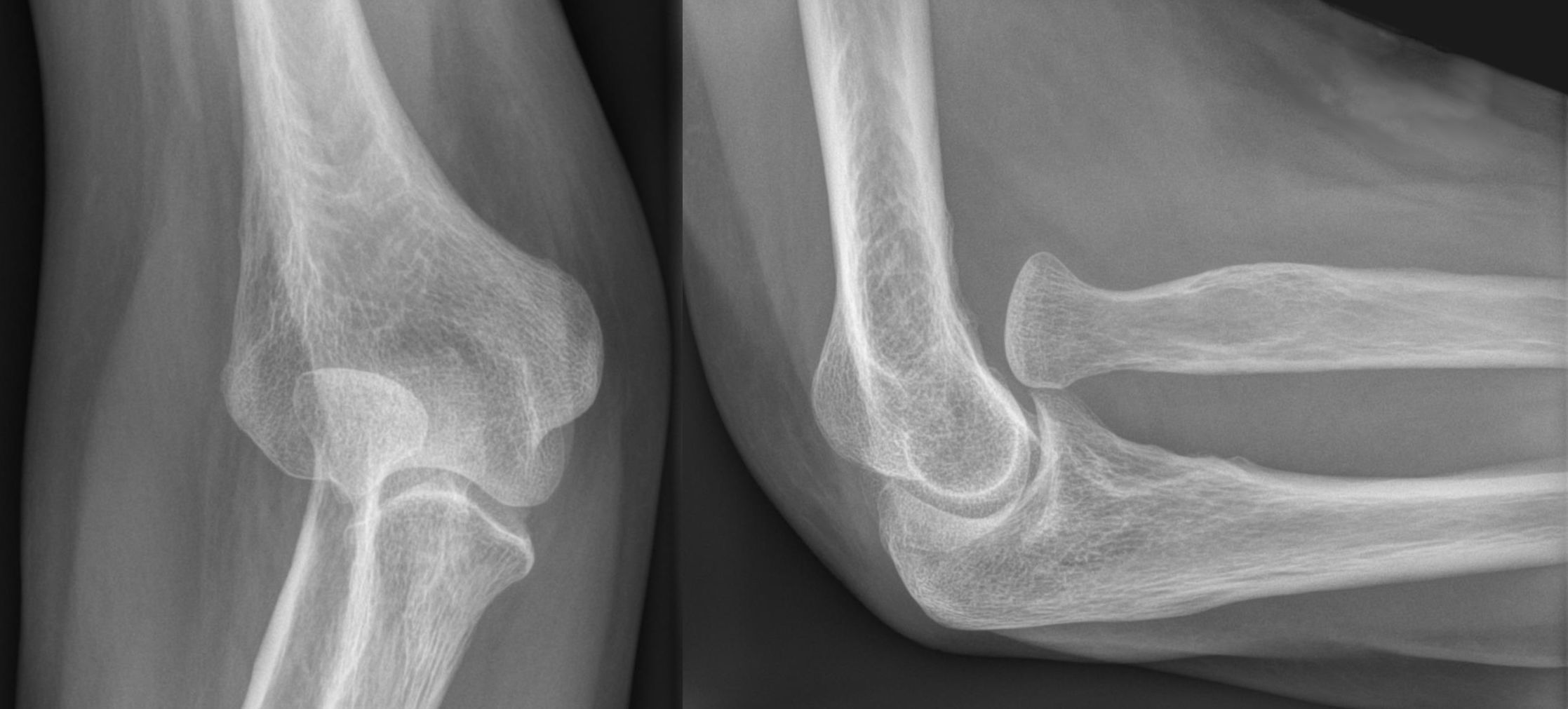
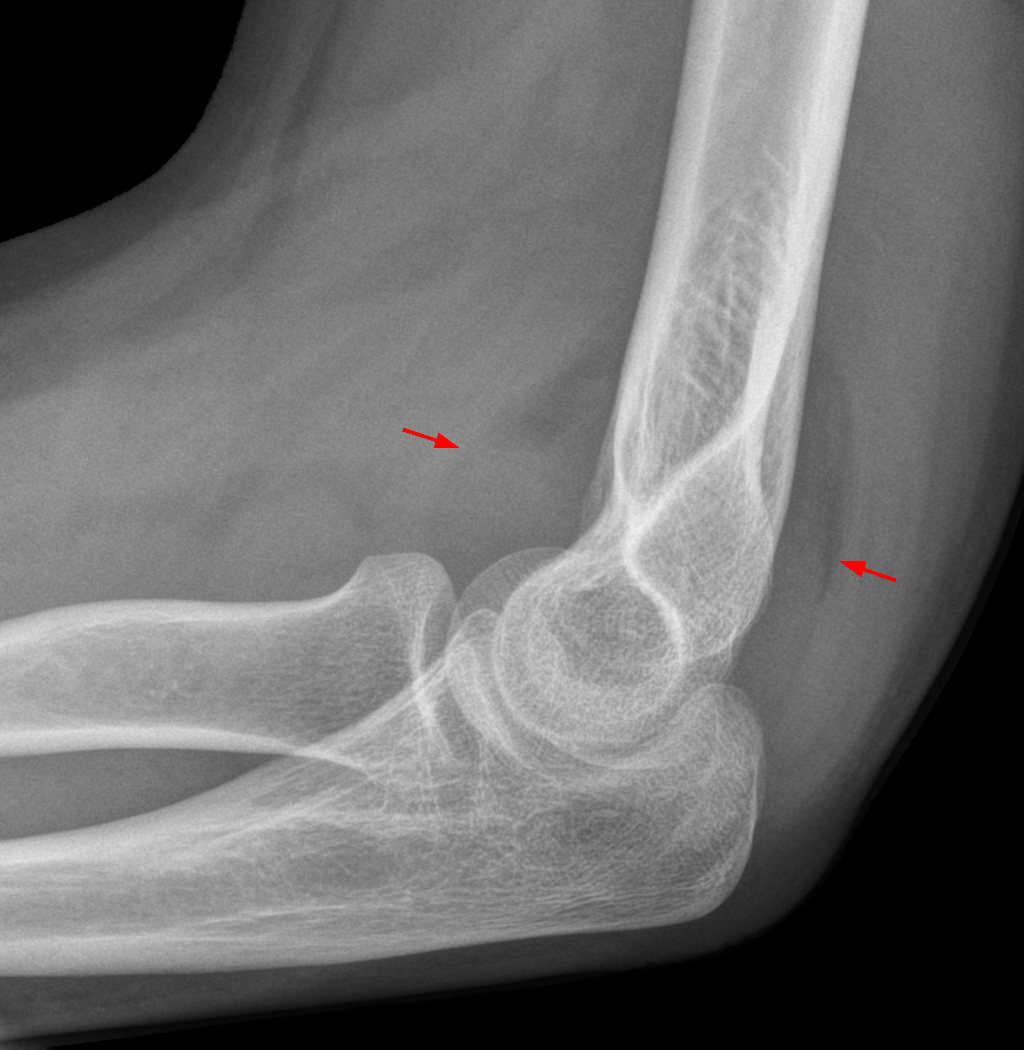
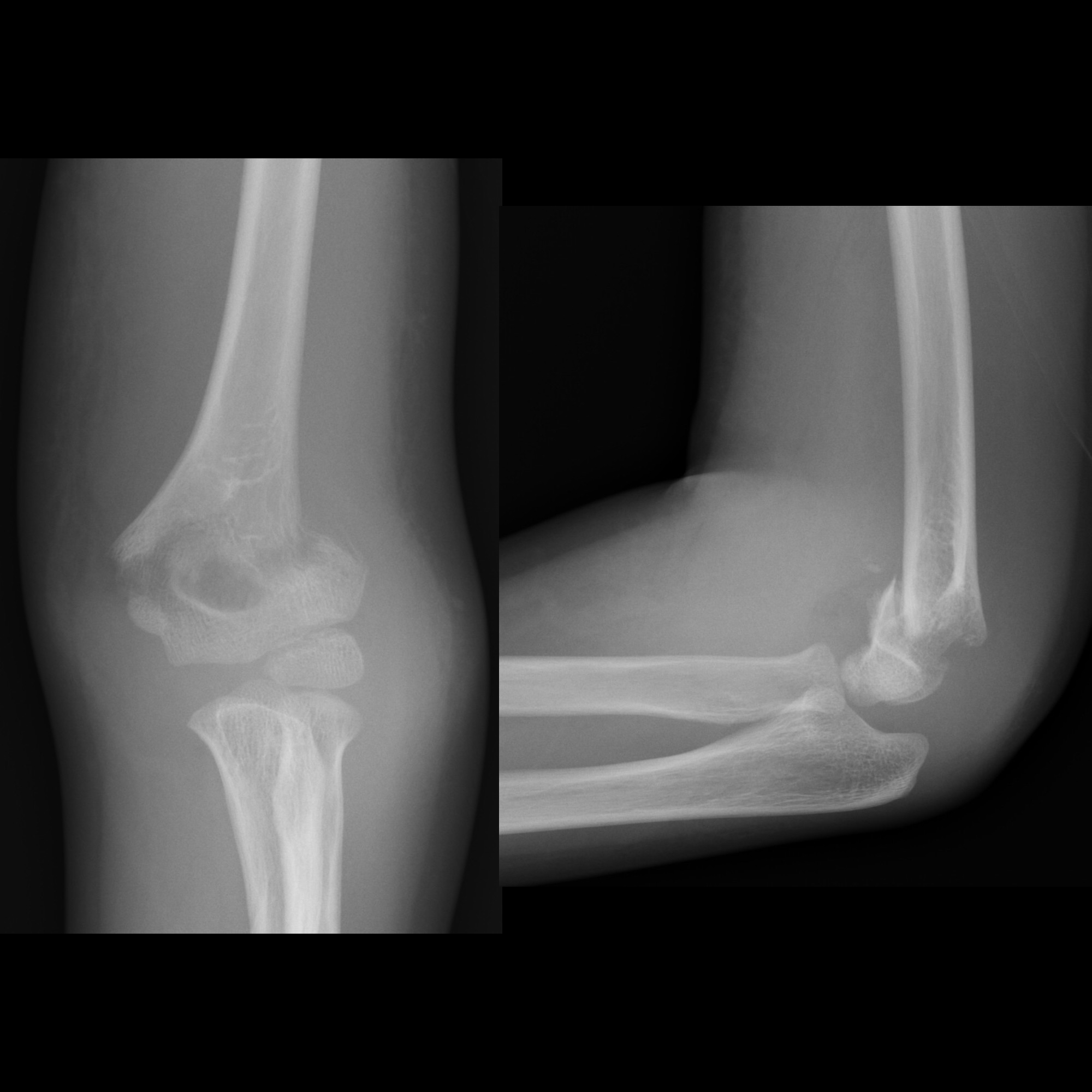
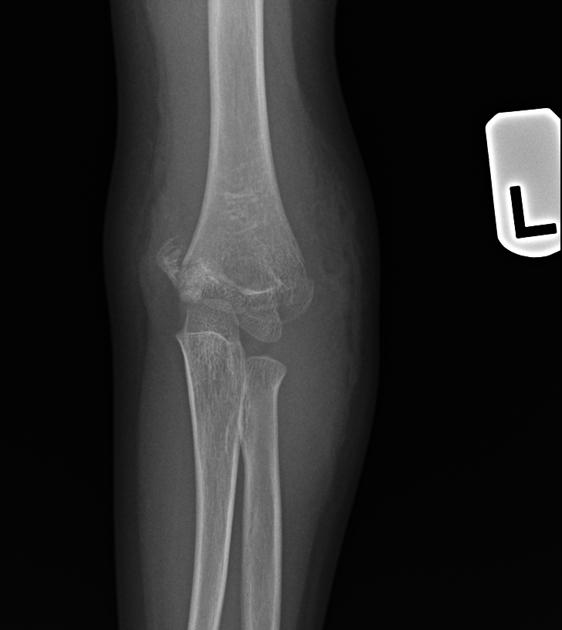
Lateral and AP radiographs are usually sufficient, and in many instances demonstrate an obvious fracture. Often, however, no fracture line can be identified. In such cases assessing for indirect signs is essential:
- anterior fat pad sign (sail sign): the anterior fat pad is elevated by a joint effusion and appears as a lucent triangle on the lateral projection
- posterior fat pad sign
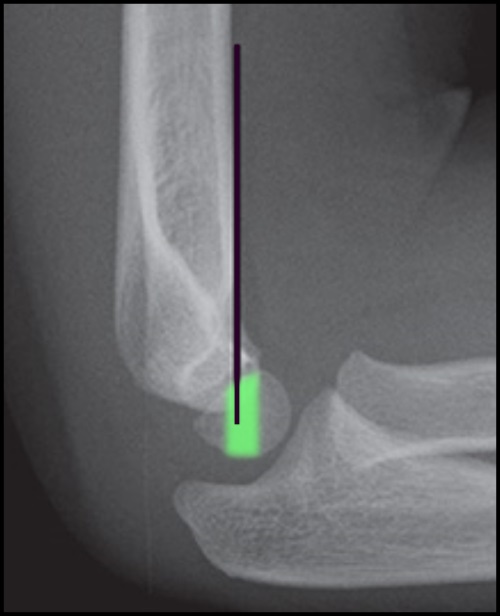
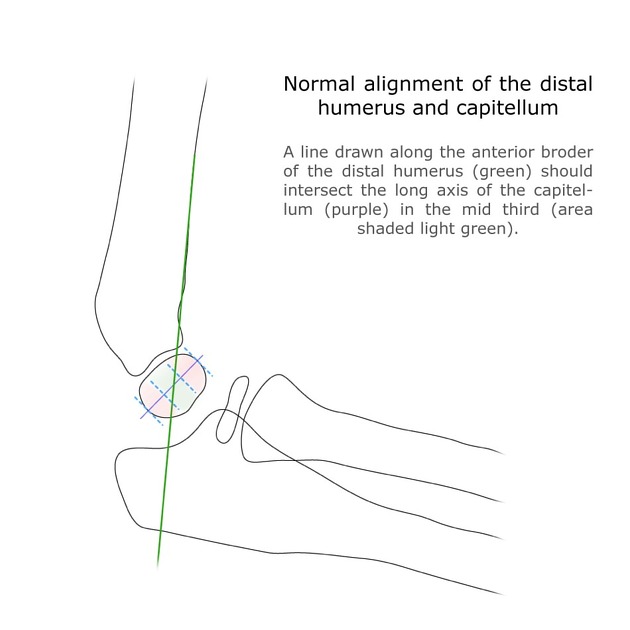
- anterior humeral line should intersect the middle third of the capitellum in most children although, in children under 4, the anterior humeral line may pass through the anterior third without injury
Radiology report
After ensuring that the films are technically adequate, assessment should include:
- description of the fracture
- location and especially presence of articular involvement
- angulation (use the anterior humeral line)
- alignment of the radius and ulna with the distal humerus
- description of additional features
- assess for joint effusion (anterior and posterior fat pad sign)
- assess alignment of the radiocapitellar joint
- remember to assess elbow centers of ossification (CRITOE)
Treatment and prognosis
Although in many cases the fracture is easily seen, in some instances all that may be seen is soft tissue swelling or an anterior fat pad sign. Even in the absence of an obvious fracture, the patient needs to be treated with a cast. Repeating radiographs after inflammation has subsided may be helpful in demonstrating the fracture; this is typically done 7-10 days later.
Management depends on the type and degree of angulation .
Type I
Type I (undisplaced) fractures are stable and can be treated with cast immobilization for approximately 3 weeks.
Type II
Type IIa usually require reduction (especially when angulation is more than 20 degrees). Although traditionally these fractures were treated non-operatively with cast immobilization of the flexed arm to 120 degrees, this however dramatically increases the risk of ischemic contracture (Volkmann contracture), as such most authors recommend percutaneous pinning (CRIF) and cast immobilization with less than 90 degrees flexion . Type IIb always required reduction +/- fixation.
Type III
Type III fractures can sometimes be treated similarly to type II (closed reduction and percutaneous pinning, CRIF) although frequently the fracture is held open by interposed soft tissues requiring open reduction .
Complications
There are three main complications :
- malunion: resulting in cubitus varus (varus deformity of the elbow, also known as gunstock deformity)
- ischemic contracture (Volkmann contracture) due to damage/occlusion to the brachial artery and resulting in volar compartment syndrome
- damage to the ulnar nerve, median nerve, or radial nerve
- most commonly insured at the time of injury is the AIN, followed by the radial nerve and then the ulnar nerve. Ulnar nerve injury is more common in flexion type fractures.
Rare complication:
- fishtail deformity due to resorption of the trochlear ossification center (or failure of formation) due to an osteonecrosis type phenomenon
Video tutorial
Siehe auch:
- Ossifikationszentren Ellenbogen
- Nervus medianus
- flexion supracondylar fracture
- Humerusfraktur
- distale Humerusfraktur
- epicondylar fracture
- vordere humerale Linie
- kindliches Ellenbogentrauma
- Radiusköpfchen-Subluxation
- CRITOE
- Gartland classification
- Classification of supracondylar fractures
- humeral condylus
- vorderes Fettpolsterzeichen Ellenbogen
und weiter:


 Assoziationen und Differentialdiagnosen zu suprakondyläre Humerusfrakturen:
Assoziationen und Differentialdiagnosen zu suprakondyläre Humerusfrakturen: