extracorporeal membrane oxygenation



Extracorporeal membrane oxygenation (ECMO) is used as a modified pulmonary or cardiopulmonary bypass technique in those with severe cardiac and/or respiratory failure refractory to conventional ventilatory support and medical intervention . There are two access paths for extracorporeal life support (ECLS) cannulation, venoarterial (VA) ECMO and venovenous (VV) ECMO, which can be performed via a surgical cut-down or percutaneous insertion.
Terminology
The basic components of an ECMO circuit are as follows:
- cannulae
- traditionally, two cannulae were introduced for blood drainage and return, respectively
- drainage cannulae are typical of a larger bore (23–31 F) compared to return cannulae (15–19 F)
- exact diameter dependent on numerous factors, including target vessel and approach
- membrane oxygenator/heat exchanger
- blood pump
- roller pumps
- centrifugal pumps
- conduit tubing
Venoarterial (VA) ECMO
The ECLS system, as VA ECMO, drains the blood from the right atrium via a femoral or internal jugular venous cannula or in patients with an open chest, directly from the right atrium. The blood is actively pumped through a membrane oxygenator, removing carbon dioxide and adding oxygen. Afterwards, the oxygenated blood is actively pumped into the arterial central system via a cannula placed in the femoral or subclavian artery (closed chest) or directly into the aorta. VA ECLS can provide full cardiopulmonary support with a high blood flow up to 6-7 L/min.
Venovenous (VV) ECMO
VV ECMO drains blood from the superior vena cava via an internal jugular venous cannula or inferior vena cava via a femoral venous cannula. The blood is pumped via the oxygenator back into the venous system via a femoral venous cannula. A double-lumen cannula, inserted in the internal jugular vein, can be used for venous drainage and return. VV ECMO can provide full or partial extracorporeal pulmonary support with blood flow up to 6 L/min.
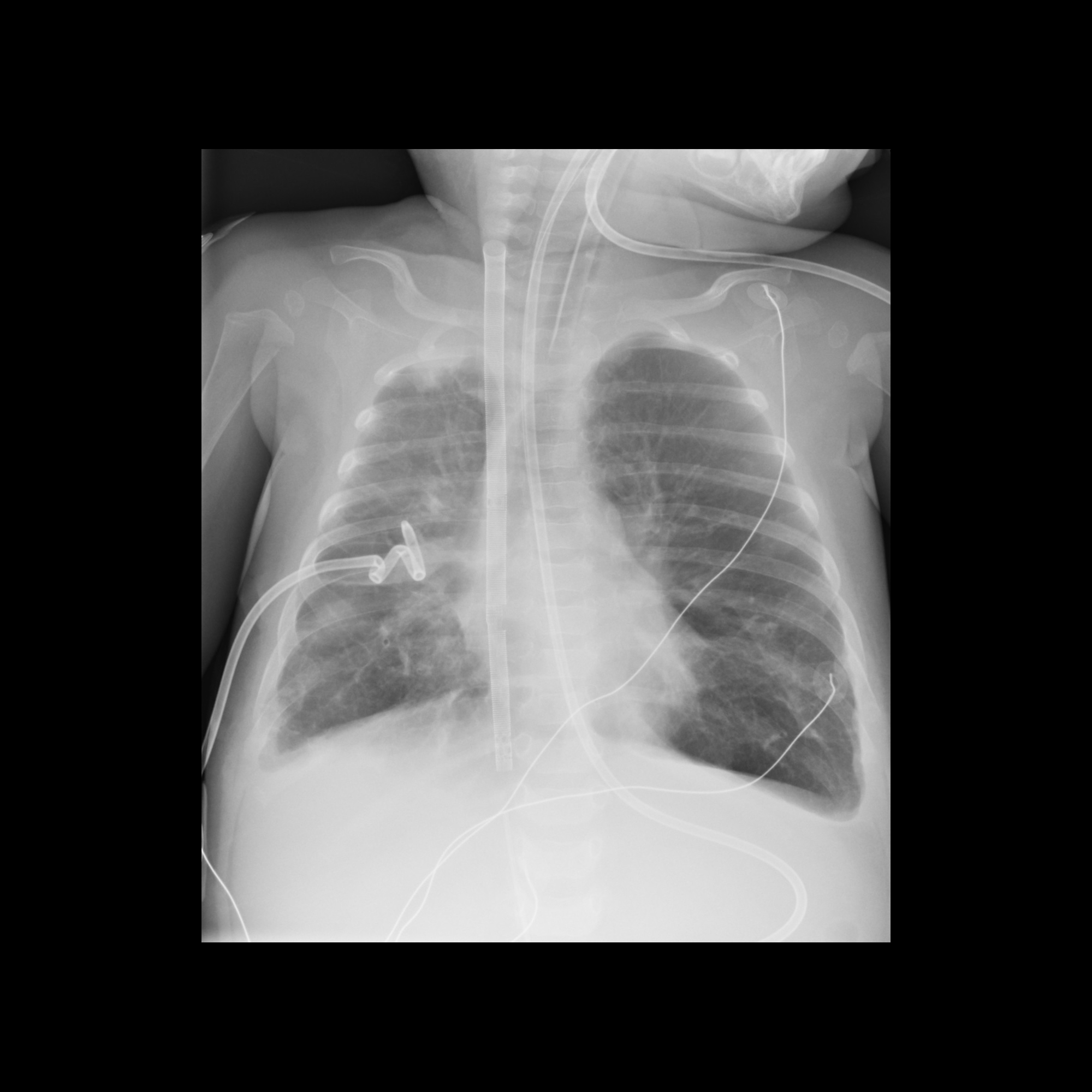
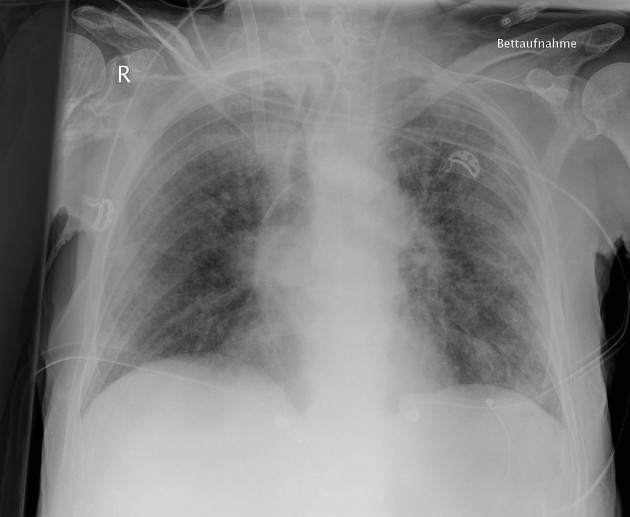
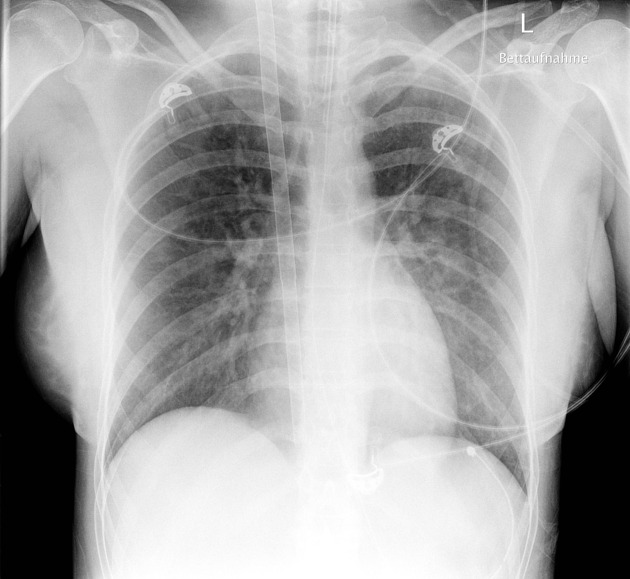
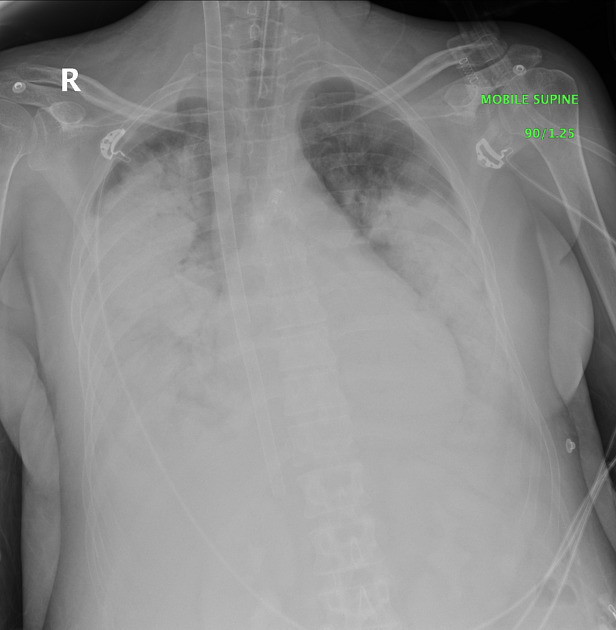
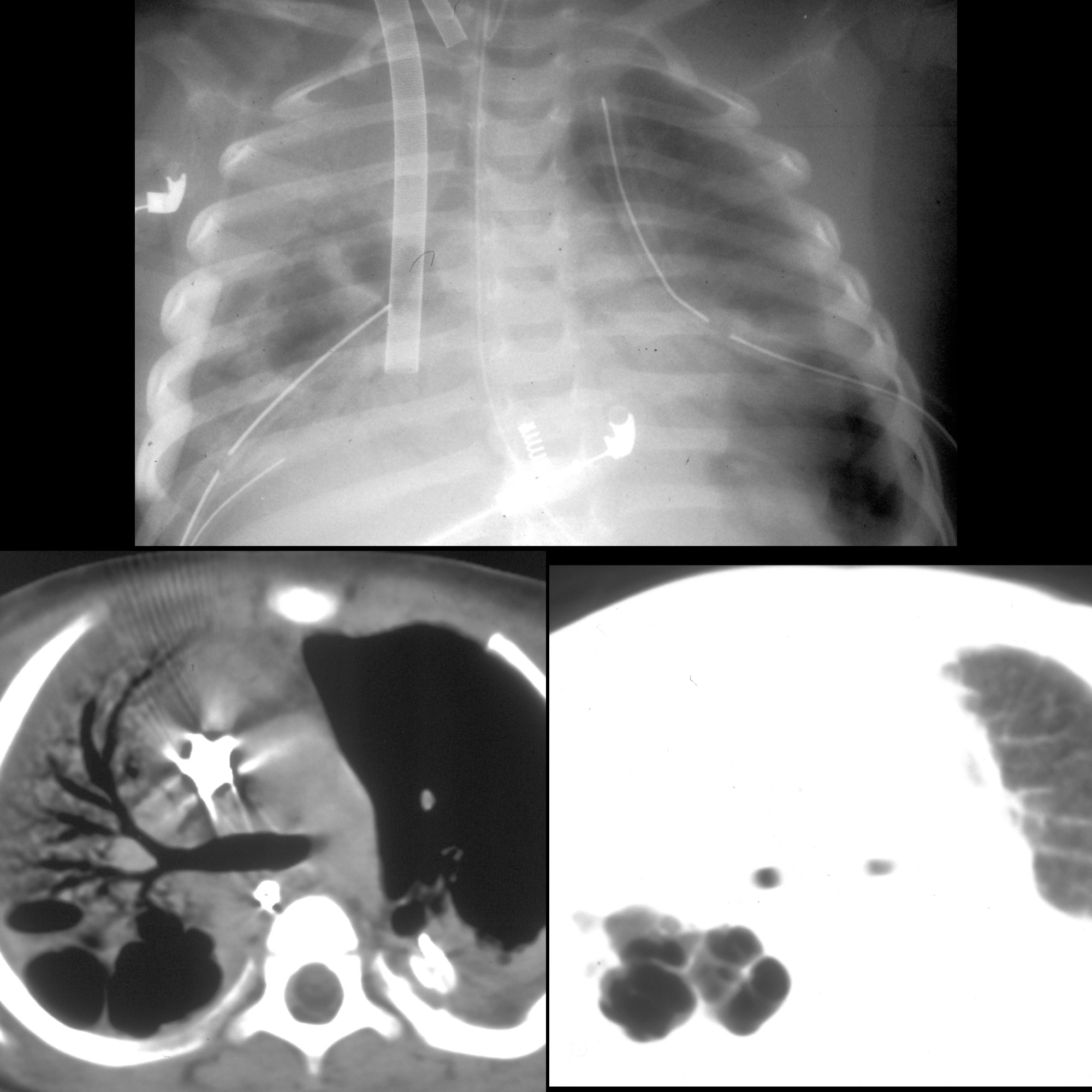
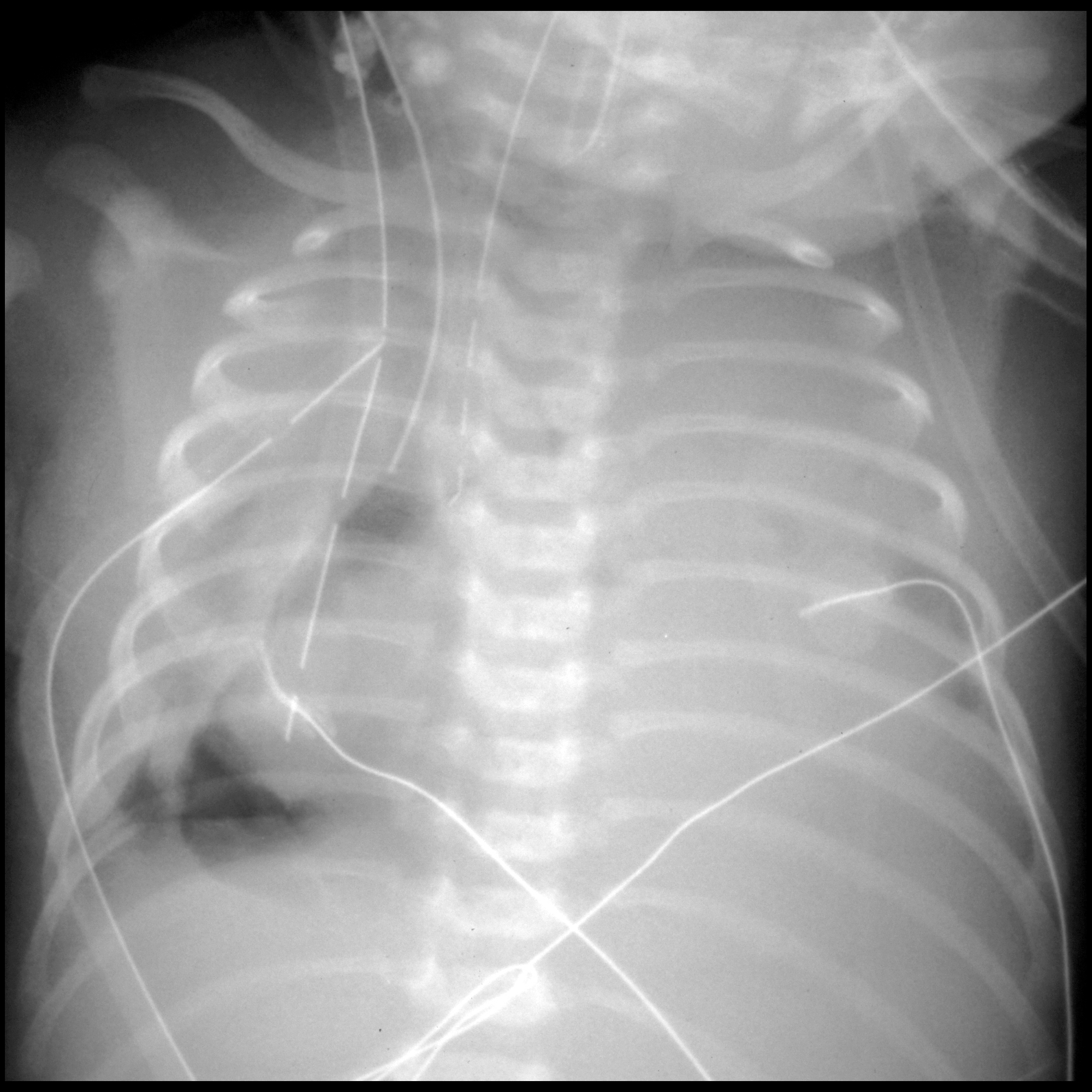
Radiographic findings
Transesophageal echocardiography
TEE has been used to guide placement of venovenous ECMO cannulation. It is most commonly employed for the placement of a bicaval double-lumen cannula, usually introduced percutaneously in the right internal jugular vein. This single cannula has ports allowing simultaneous drainage of deoxygenated blood from the IVC and SVC, with a return lumen that should be angulated so that flow travels through the tricuspid valve into the right ventricle .
- mid-esophageal bicaval view
- using the Seldinger technique, a wire is advanced from the right internal jugular vein toward the inferior vena cava
- the bicaval view allows visualization of the wire as it courses from the SVC to the IVC across the right atrium in the sonographic far field, thus excluding accidental intraventricular misplacement
- inadvertent placement of the guidewire in the right ventricle may result in complications such as;
- ventricular free wall rupture
- cardiac tamponade
- inadvertent placement of the guidewire in the right ventricle may result in complications such as;
- modified transgastric position
- probe may be advanced to visualize the wire tip terminating in the IVC below the hepatic veins
- modified midesophageal bicaval view
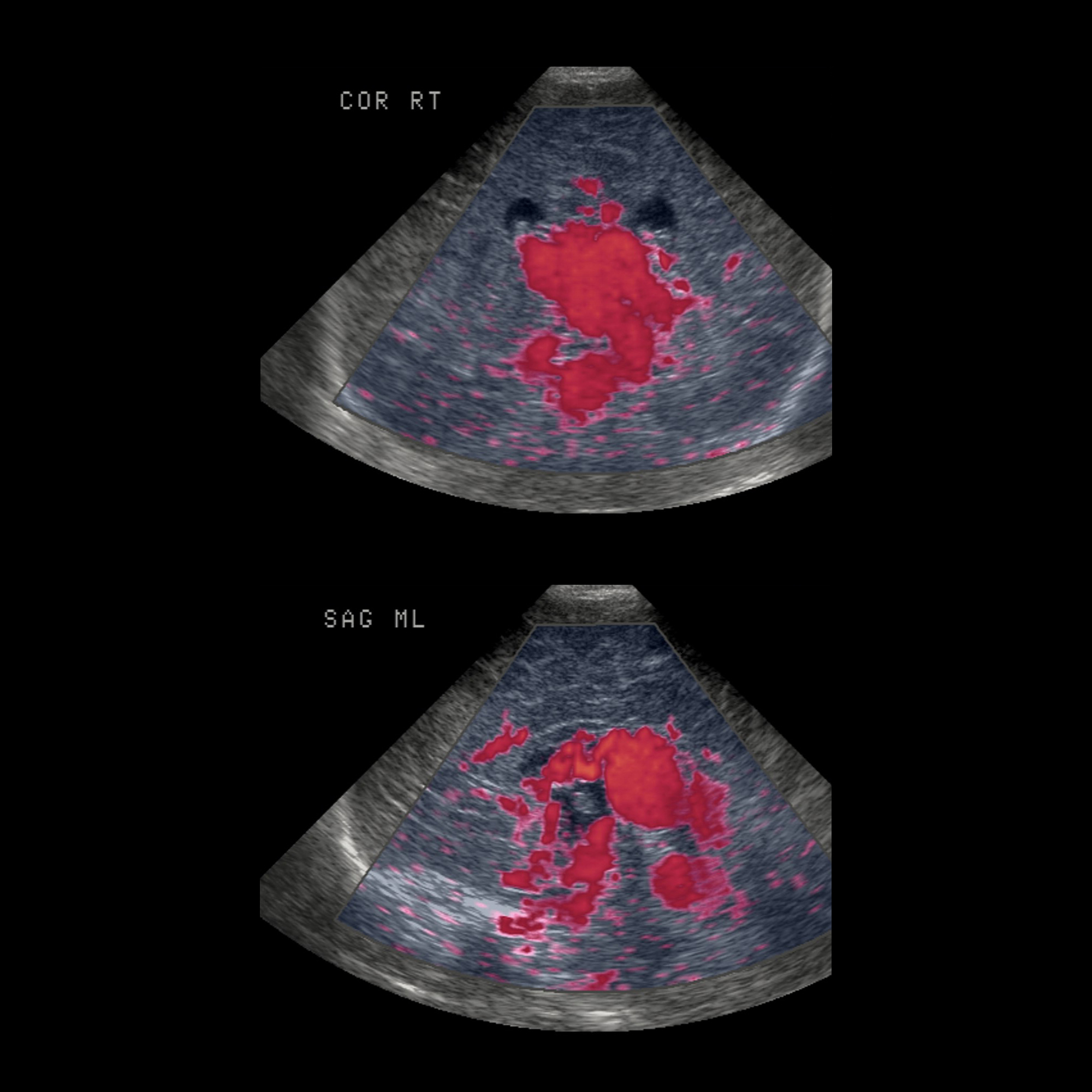
- once the catheter has been advanced, the probe may be withdrawn and color flow Doppler interrogation of the side port of the ECMO cannula may be used to assess the appropriateness of the return port orientation
- correct placement is suggested by an aliased color jet coursing toward the tricuspid valve originating from a catheter placed in the right atrium
- transthoracic subcostal windows may complement this assessment, demonstrating normal antegrade hepatic venous Doppler flow
Transesophageal echocardiography
Contrast-enhanced CT examinations of patients undergoing ECMO presents unique technical and diagnostic challenges. A number of considerations can be explored here.
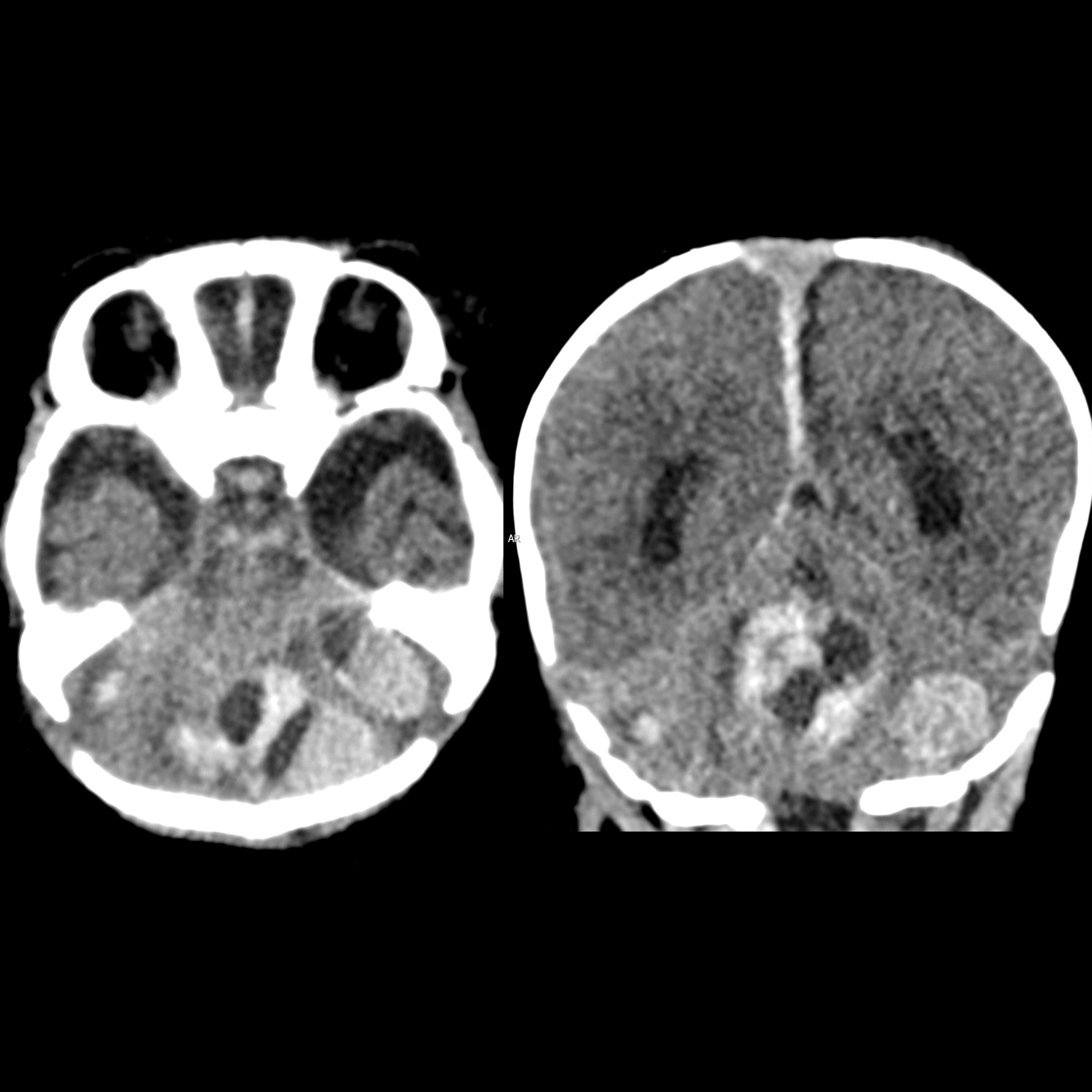
Complications
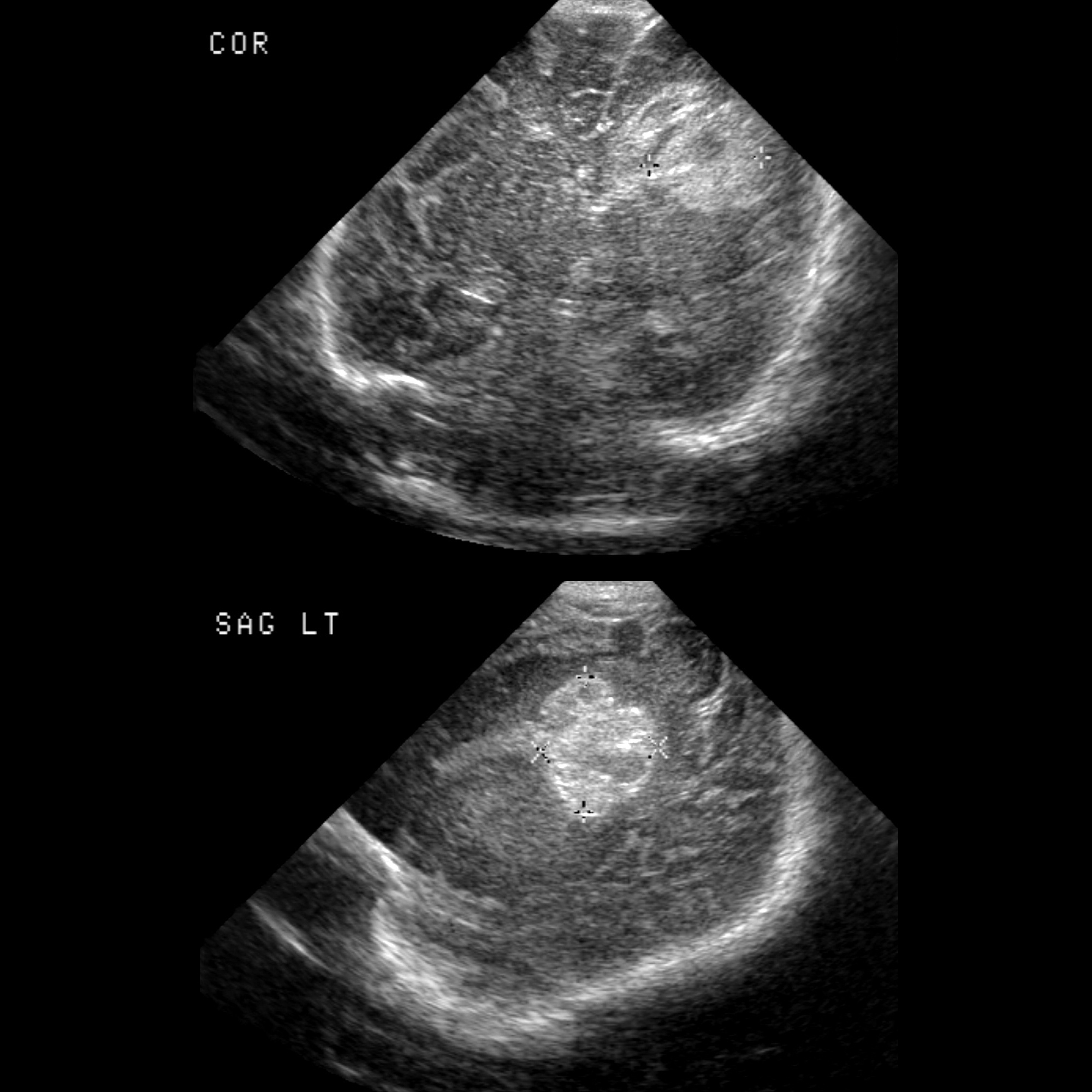
- intracranial hemorrhage from anticoagulation
- migration of support apparatus
- gas collections
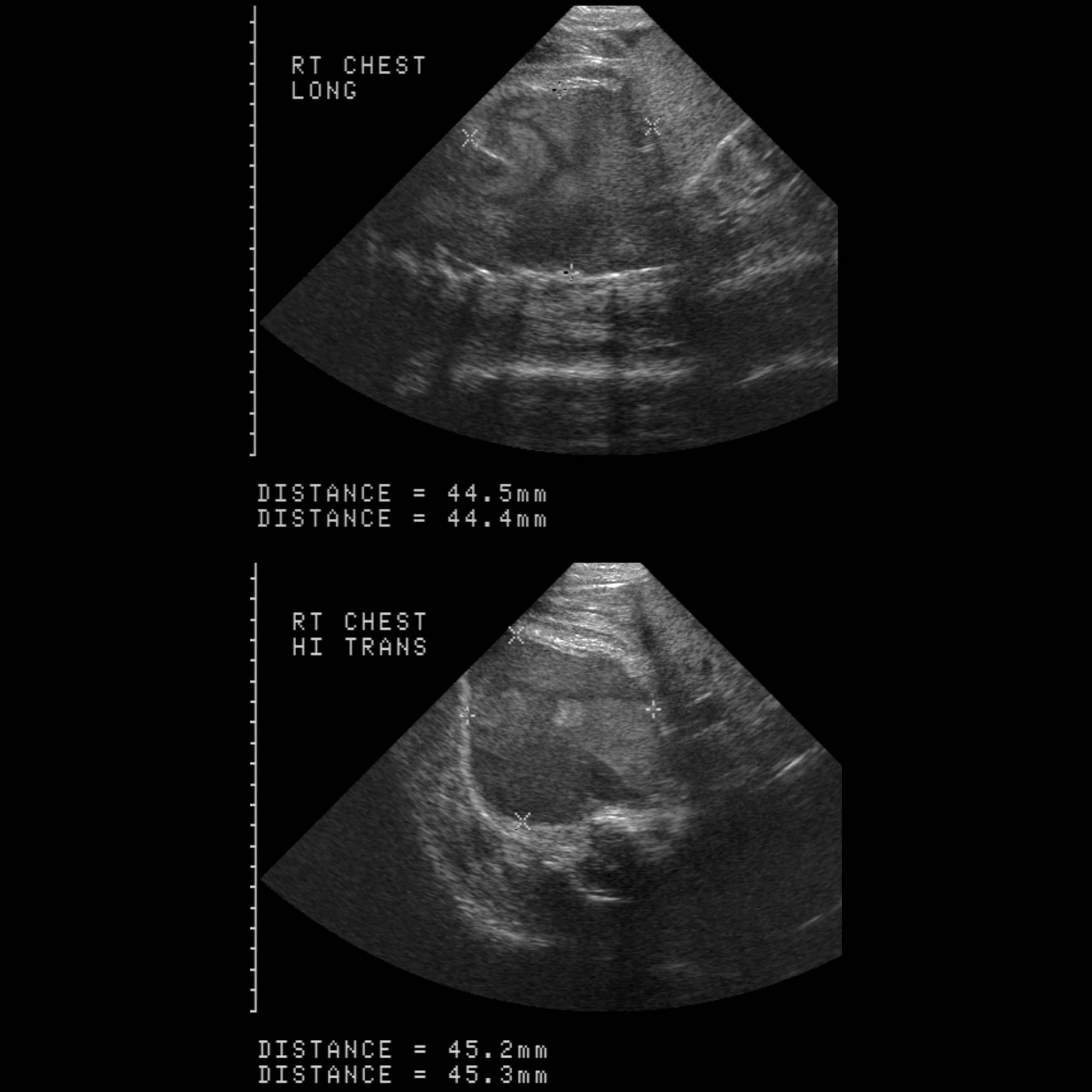
- pleural effusion
- pulmonary hemorrhage
- adrenal hemorrhage
- intraperitoneal hemorrhage
- hepatic infarction
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Extrakorporale Membranoxygenierung:
Assoziationen und Differentialdiagnosen zu Extrakorporale Membranoxygenierung:
