Guillain-Barre syndrome


Guillain-Barré syndrome (GBS) is a heterogeneous group of autoimmune polyradiculopathies, involving sensory, motor, and autonomic nerves. It is the most common cause of rapidly progressive flaccid paralysis. It is believed to be one of a number of related conditions, sharing a similar underlying autoimmune abnormality, collectively known as anti-GQ1b IgG antibody syndrome.
Epidemiology
Most cases are preceded by upper respiratory tract infections or diarrhea one to three weeks before their onset, most commonly caused by Campylobacter jejuni (25-40% of patients are seropositive) . Molecular mimicry with the bacterial agents is thought to cause the autoimmunity with the development of anti-GQ1b IgG antibodies.
Other predisposing factors include recent surgery, lymphoma, and systemic lupus erythematosus (SLE) .
Clinical presentation
The classical presentation of Guillain-Barré syndrome includes symmetrical ascending muscle paresis/paralysis, areflexia/hyporeflexia, and variable sensory or autonomic involvement.
Several subtypes have been described including:
- acute inflammatory demyelinating polyradiculoneuropathy (AIDP)
- most common form (60-90%)
- axonal subtypes
- acute motor axonal neuropathy (AMAN) / Chinese paralytic syndrome
- acute motor-sensory axonal neuropathy (AMSAN)
- both axonal subtypes are thought to be due to antibodies to gangliosides which result in macrophages invading the axons at the nodes of Ranvier
- regional GBS syndromes
- Miller Fisher variant (MFS/MFV)
- characterized by ataxia, ophthalmoplegia, and areflexia without weakness
- anti-GQ1b antibodies are present in most cases
- polyneuritis cranialis
- Miller Fisher variant (MFS/MFV)
Guillain-Barré syndrome is diagnosed by the combination of clinical presentation, CSF study, and electrophysiological criteria.
CSF abnormalities are characterized by increased protein without pleocytosis, which is a non-specific finding, seen in many of the conditions which mimic GBS on imaging and clinically .
Nerve conduction abnormalities include slow or blocked nerve conduction, prolongation of distal latency, and f-waves.
Chronic inflammatory demyelinating polyneuropathy (CIDP) is considered the chronic counterpart to Guillain-Barré syndrome.
Radiographic features
Radiological studies are requested to exclude other causes and in cases where nerve conduction studies and CSF examination are equivocal. MRI of the spine is most useful, helping to exclude other etiologies, such as transverse myelitis and compressive causes of polyradiculopathy.
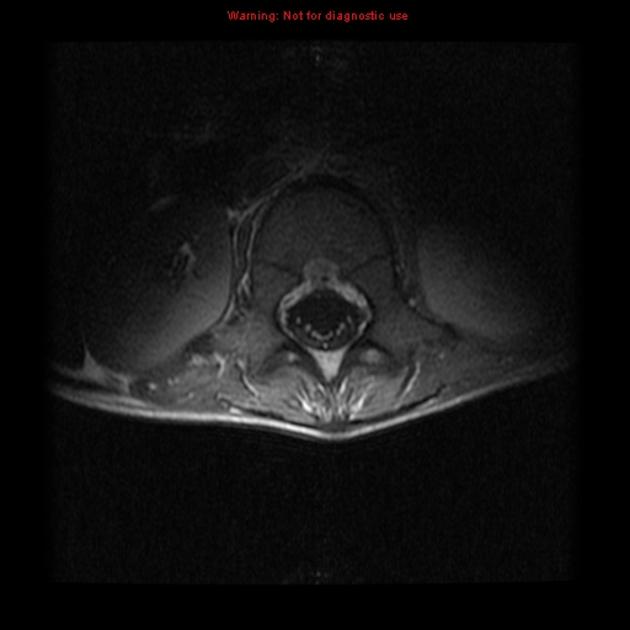
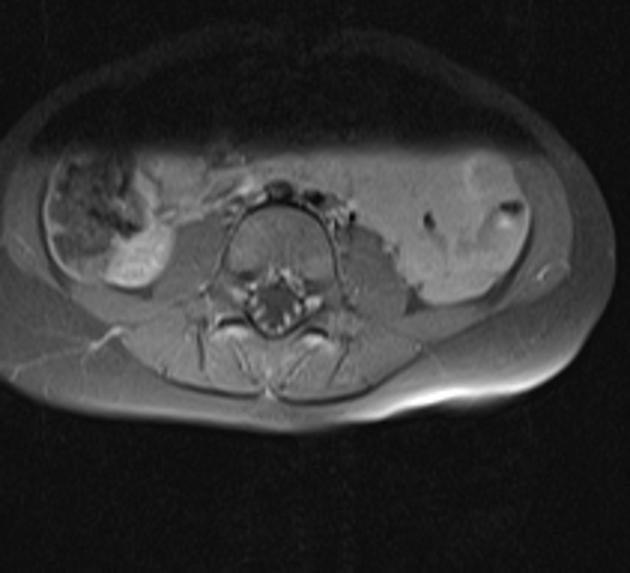
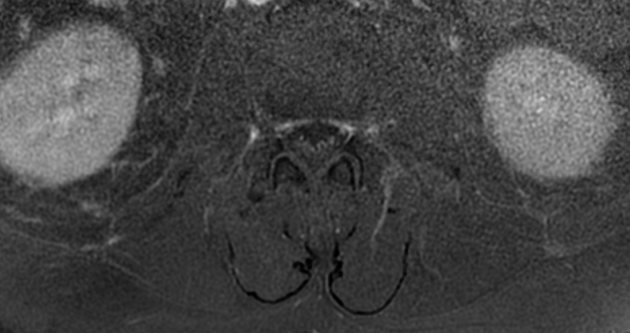
MRI
It is essential that contrast is administered if the diagnosis is suspected as non-contrast sequences are essentially normal .
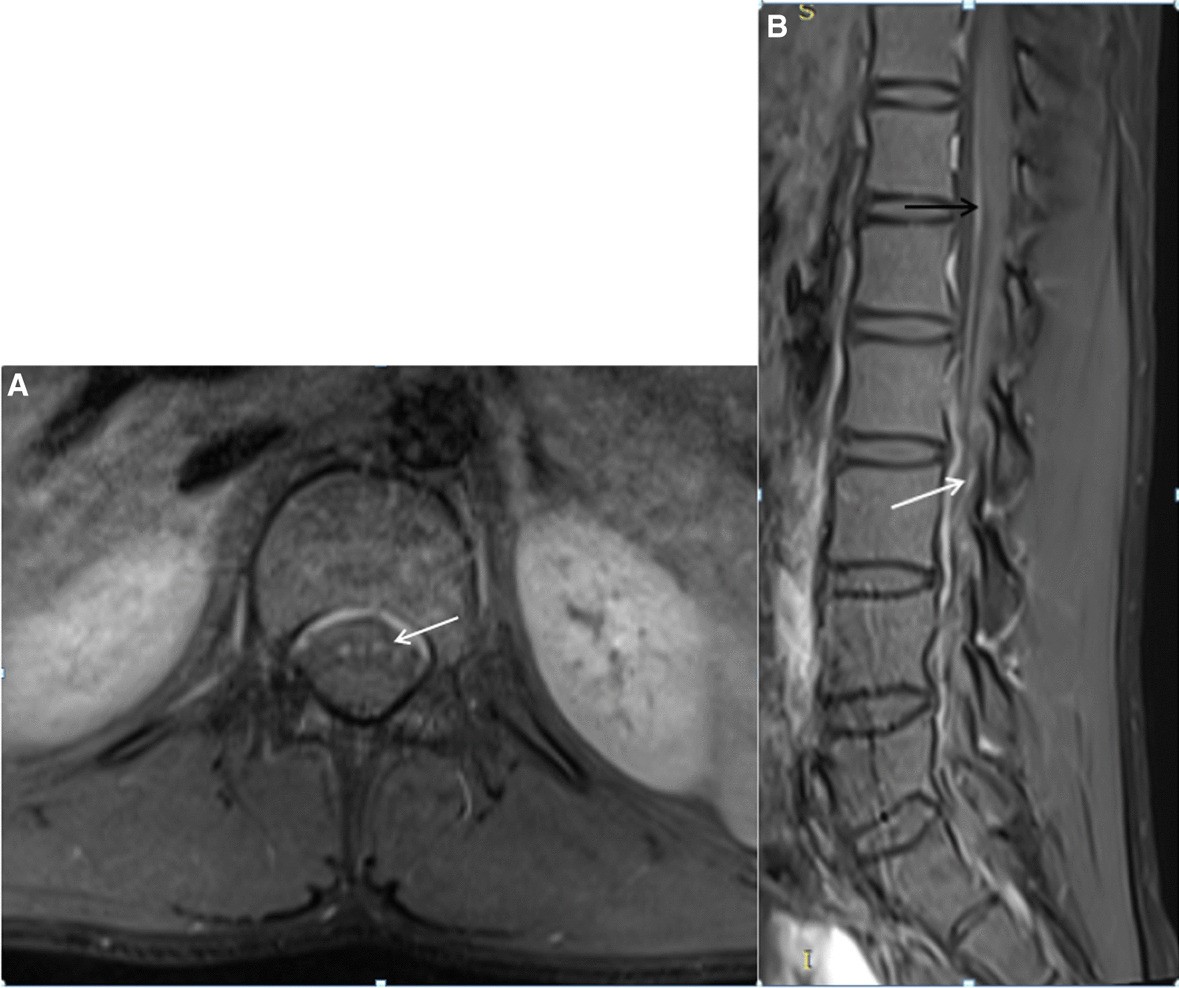
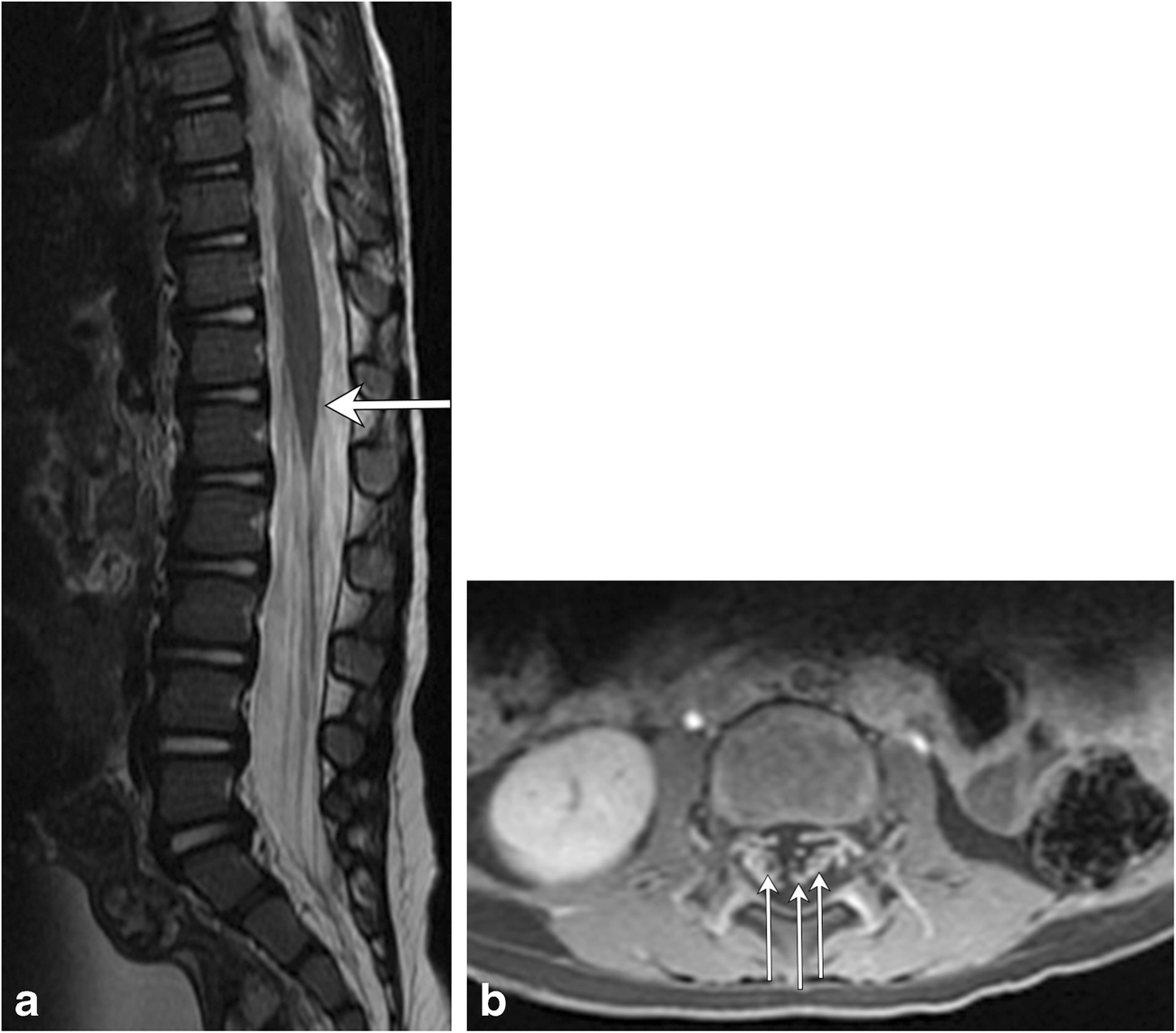
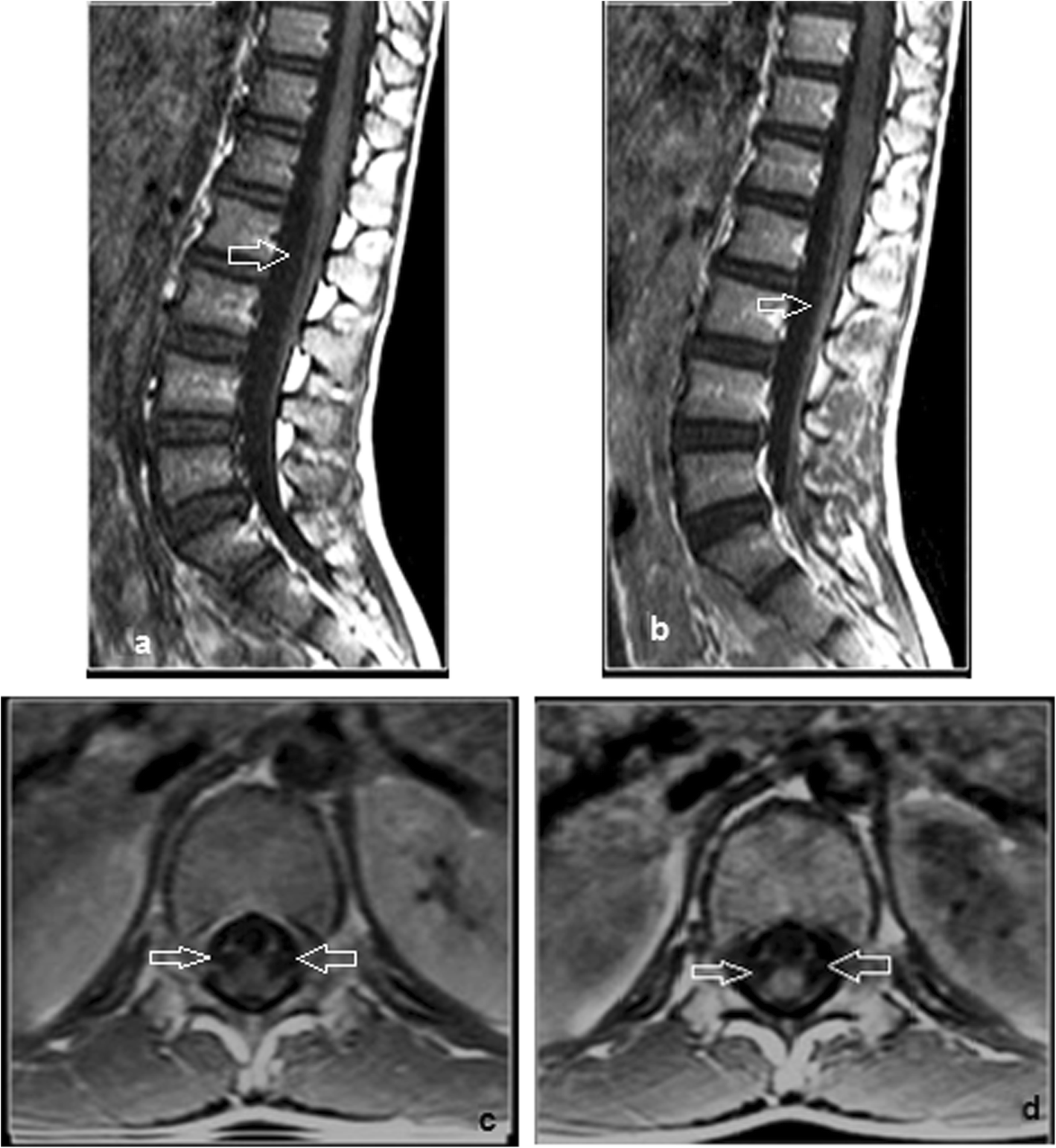
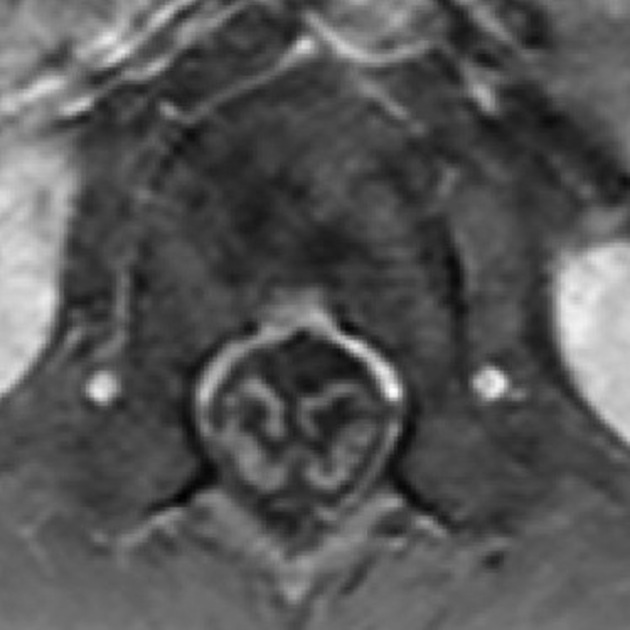
Typical findings in Guillain-Barré syndrome are surface thickening and contrast enhancement on the conus medullaris and the nerve roots of the cauda equina .
The most common site of enhancement in Guillain–Barré syndrome is considered to be anterior nerve roots, although enhancement of the posterior nerve roots is also seen .
In the brain, the facial nerve (CN VII) is the most commonly affected cranial nerve .
Treatment and prognosis
Guillain-Barré syndrome is primarily managed with IV immunoglobulin or plasmapheresis along with supportive measures, which can speed up recovery . Typically improvement occurs after a number of weeks to months although there is significant mortality (3-10%) .
History and etymology
The syndrome was named after Georges Charles Guillain (1876-1961) and Jean Alexandre Barré (1880-1967), French neurologists. André Strohl (1887-1977), a French physiologist, worked together with both neurologists and is the third author in the description done in 1916, and for this reason, the syndrome is also referred to as Guillain-Barré-Strohl syndrome.
Differential diagnosis
The differential is essentially that of nerve root/cauda equina enhancement:
- AIDS-related polyradiculopathy
- arachnoiditis from any cause (e.g. postoperative, or post intrathecal injection)
- neurosarcoidosis
- leptomeningeal carcinomatosis and lymphoma
- chronic inflammatory demyelinating polyneuropathy (CIDP)
- acute presentation of CIDP can be similar to GBS
- difficult to differentiate in the first 6 weeks
- after 6-8 weeks GBS should be improving whereas CIDP will demonstrate chronic inflammation
- Lyme disease
- rabies encephalitis (paralytic variant): similar presentation, but more fulminant course resulting in rapid demise in almost all cases
Siehe auch:
- Neurosarkoidose
- chronisch adhäsive Arachnopathie
- chronische inflammatorische demyelinisierende Polyneuropathie
- Miller-Fisher-Syndrom
- acute motor axonal neuropathy
- Polyradikuloneuropathie
und weiter:


 Assoziationen und Differentialdiagnosen zu Guillain-Barré-Syndrom:
Assoziationen und Differentialdiagnosen zu Guillain-Barré-Syndrom:
