Harnleiterstein
















Ureteric calculi or stones are those lying within the ureter, at any point from the ureteropelvic junction (UPJ) to the vesicoureteric junction (VUJ). They are the classic cause of renal colic-type abdominal pain. They are a subtype of the broader pathology of urolithiasis.
Epidemiology
The lifetime prevalence of ureteric calculi is relatively high, occurring in approximately 12% of men and 7% of women . The risk is increased with a past history of ureteric calculi and with positive family history. Most patients present between ages 30 and 60 years , with peak incidence between ages 35-45. Initial calculus presentation occurring past age 50 is uncommon.
Clinical presentation
Patients with ureteric calculi may present with peristaltic pain (renal colic), hematuria, nausea and vomiting.
The quality and location of pain are dependent on the location of the calculi within the ureter. Calculi within the ureteropelvic junction may cause deep flank pain due to distension of the renal capsule, without radiation to the groin, whereas pain from upper ureteral calculi radiates to the flank and lumbar areas. Calculi in the mid-ureter result in pain radiating anteriorly and caudally which may mimic appendicitis (on the right side) and diverticulitis (on the left side), while pain from distal ureteric calculi radiates to the groin via referred pain from the genitofemoral or ilioinguinal nerves.
Calculi in the ureterovesical junction may also cause irritative voiding symptoms such as dysuria and urinary frequency.
Pathology
Up to 80% of renal calculi are formed by calcium stones . Other types include struvite, uric acid and cystine stones. In specific patient groups, mucoprotein (matrix), xanthine or indinavir (and other drug-related) stones may be (rarely) encountered.
Calculi formation is likely due to two mechanisms. The first is where stone-forming substances such as calcium or uric acid supersaturate the urine beginning crystal formation. The other mechanism depends on stone-forming substances depositing in the renal medullary interstitium forming a Randall plaque and eventually eroding into the papillary urothelium, creating a calculus.
In addition to history of prior ureteric calculi and family history, other risk factors for ureteric calculi include low fluid intake, frequent urinary tract infections and medications that may crystallize within the urine.
Radiographic features
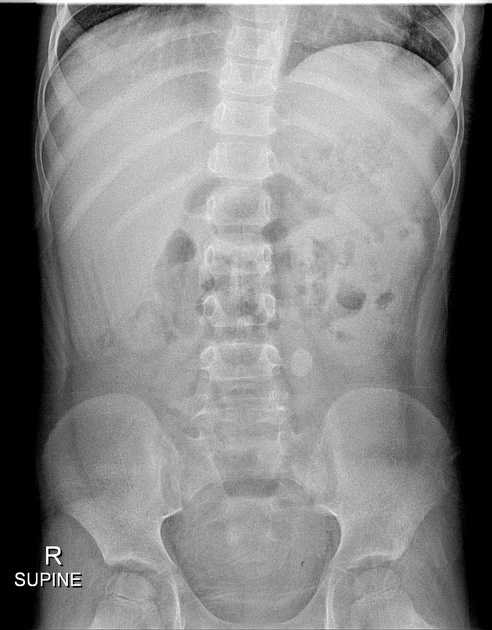
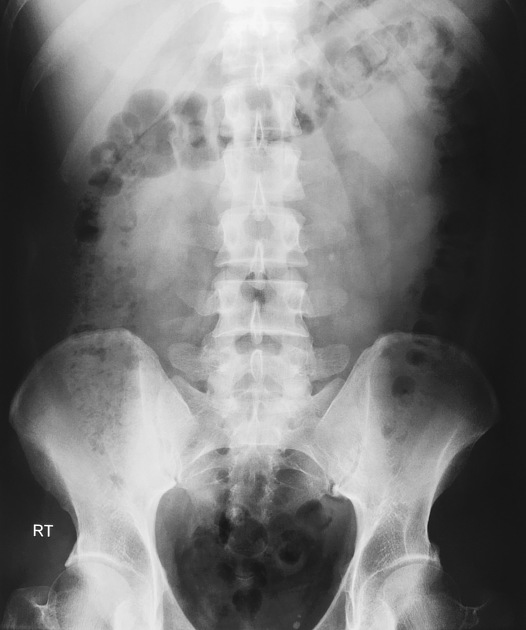
Plain radiograph
A plain abdominal (KUB) film can identify large radiopaque calculi. However, smaller calculi and/or radiolucent stones may go undetected. Obstruction/hydronephrosis cannot be adequately assessed.
For low-dose initial investigation, plain film with ultrasound is used in some centers for specific patient groups. For follow up, plain film is useful when a stone has been demonstrated on abdominal x-ray and/or CT scanogram.
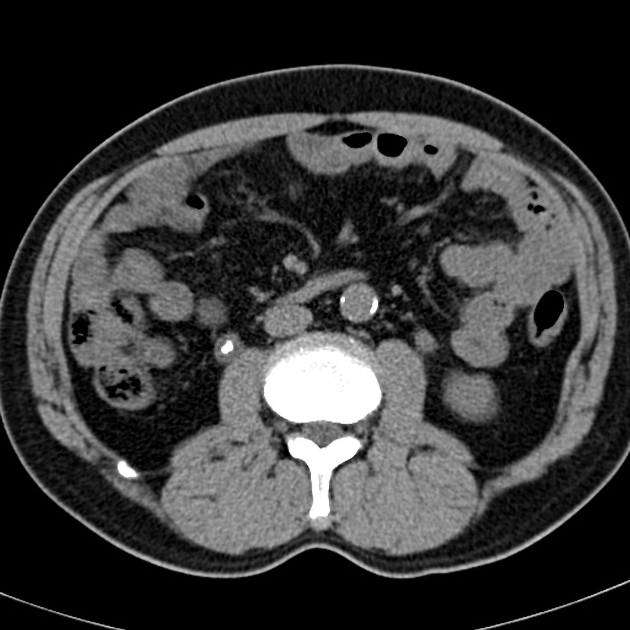
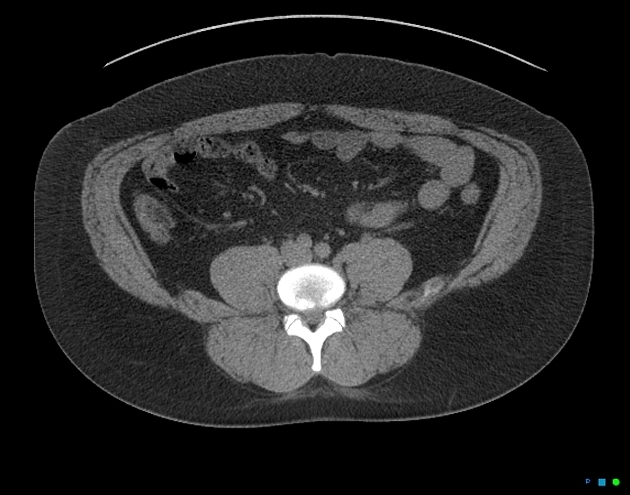
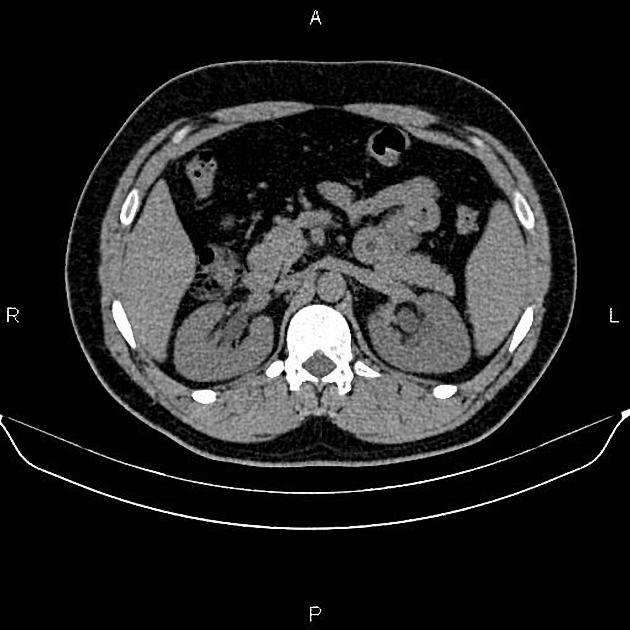
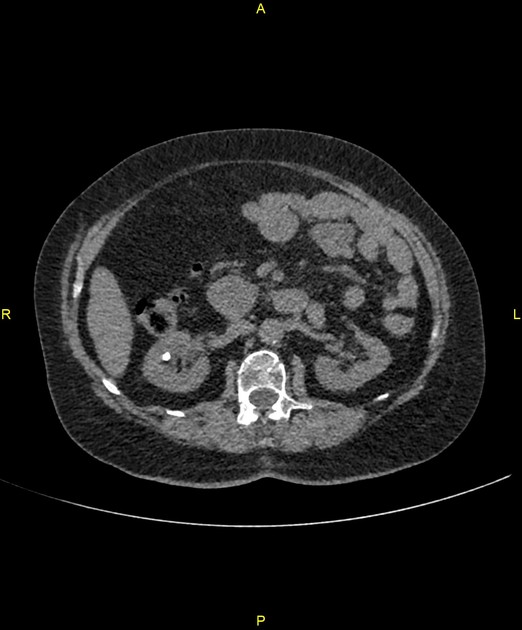
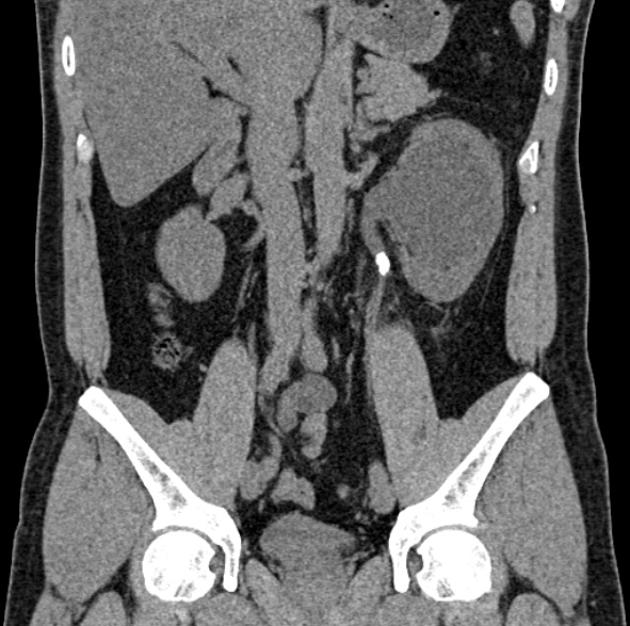
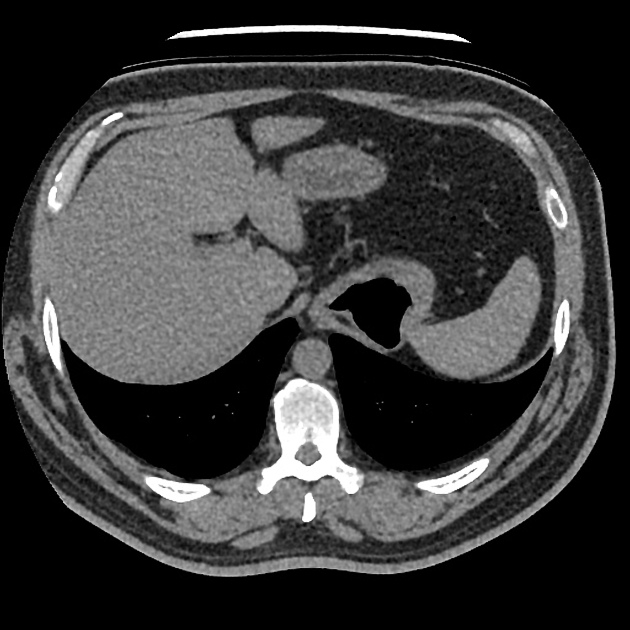
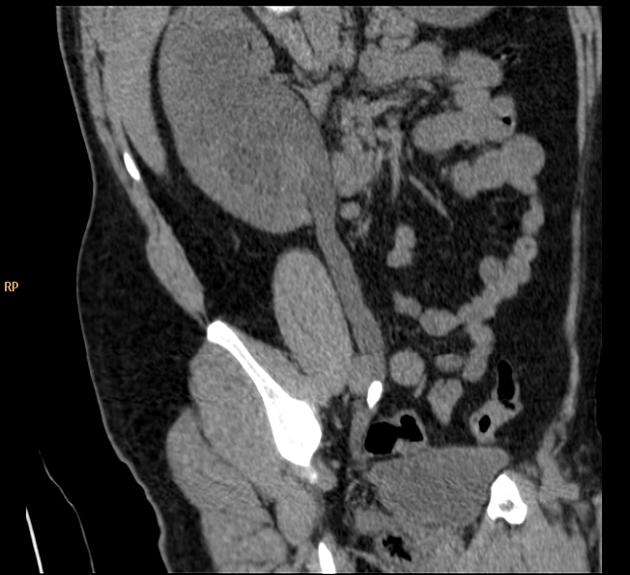
CT
Non-contrast CT (CT KUB) is the gold standard for imaging ureteric stones, with the vast majority (99%) being radiodense. Stones >1 mm in size are visualized, with the specificity of helical CT as high as 100% .
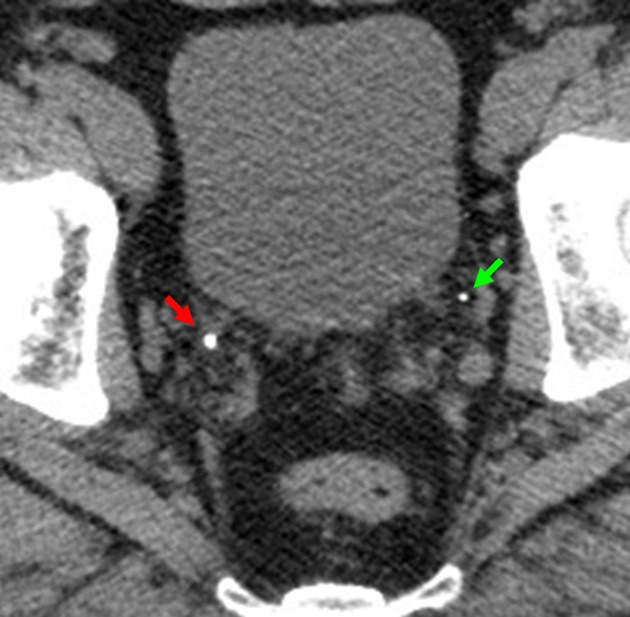
Scanning the patient in the prone position is preferred as this gives certainty as to whether a stone remains impacted within the ureterovesical junction or if it has passed freely into the bladder . A stone will always fall dependently and sit along the anterior bladder wall once it is free of the ostium in a prone patient. Alternatively, some centers will 'flip' the patient and re-scan the pelvis if a stone is identified at the ureterovesical junction/bladder base on the supine scan. The choice is often one of practicalities depending on the list supervision and staff involved.
CT KUB can also detect secondary signs of urinary tract obstruction, including ureterohydronephrosis and perinephric stranding.
In patients with little pelvic fat, distinguishing a ureteric calculus from a phlebolith can be challenging. Two signs have been found helpful:
- comet-tail sign: favors a phlebolith
- soft-tissue rim sign: favors a ureteric calculus
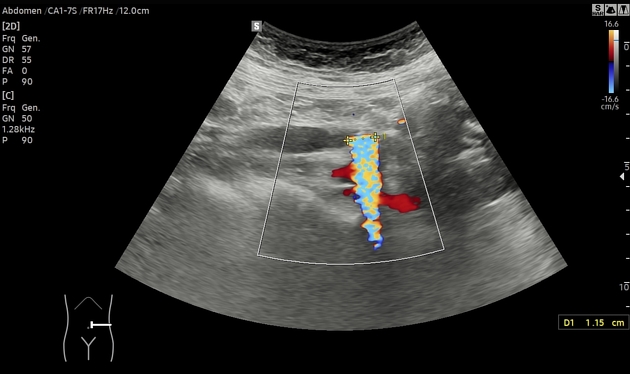
Ultrasound
While CT is the gold standard test, there is recent evidence that screening patients with ultrasound in the emergency department can help avoid CT in more than half of patients leading to reduced cumulative radiation dose without increasing complications, pain scores, emergency department visits or hospitalizations .
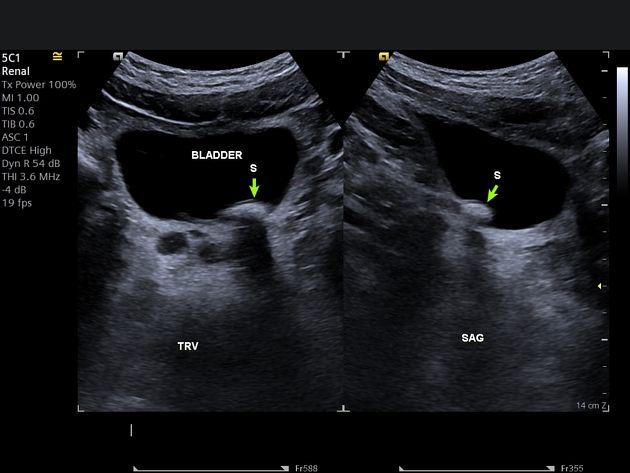
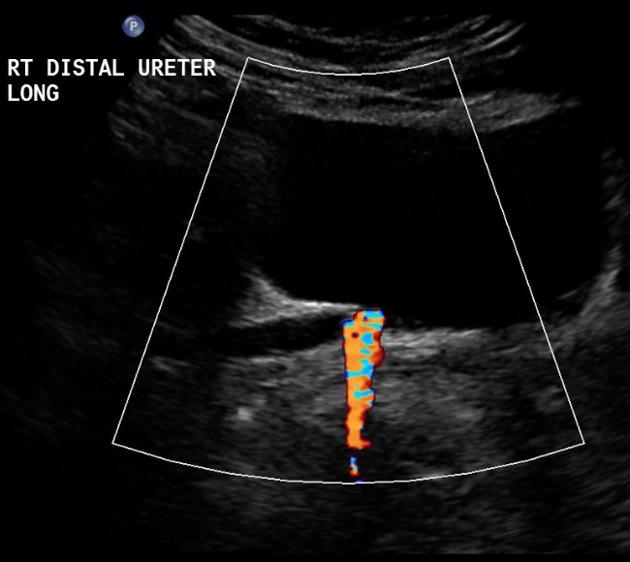
Ultrasound may be used for patients who need to avoid radiation, such as pregnant women. It is also useful for assessing for complications, such as hydronephrosis or pyonephrosis and in aiding percutaneous nephrostomy tube insertion in septic patients. Features include:
- echogenic foci
- acoustic shadowing
- twinkle artefact on color Doppler
- color comet-tail artefact
Treatment and prognosis
Most patients presenting with acute renal colic due to ureteric calculi can be managed conservatively with hydration and analgesia until the calculi pass. NSAIDs are as effective as opioids . Hospitalization may be required where oral analgesia is insufficient, in patients with a solitary kidney or in patients with urosepsis or acute kidney failure.
Calculus size and location as well as ureter anatomy are important factors in determining the likelihood of spontaneous calculus passage . Spontaneous passage by 20 weeks has been reported at the following rates (axial dimension) :
- 0-3 mm: 98%
- 4 mm: 81%
- 5 mm: 65%
- 6 mm: 33%
- >6.5 mm: 9%
However, even small calculi may be impossible to pass if they are located at the ureteropelvic junction or in patients with ureteral strictures. Passage of calculi may be facilitated by tamsulosin and nifedipine.
In calculi >10 mm or with failed conservative management, urological procedures such as extracorporeal shockwave lithotripsy (ESWL), ureteroscopic lithotripsy, or percutaneous nephrostomy may be required.
Once the calculus is passed it, should be sent for analysis to evaluate for possible underlying causes of stone disease and better plan for future prevention.
Practical points
It is good practice to report if the calculus is visible on the scanogram of the study to establish if a plain radiograph is sufficient for follow up purposes rather than a higher radiation CT study.
Differential diagnosis
- foreign body
- ureteral wall calficiation
Siehe auch:
- prävesikaler Harnleiterstein
- Phlebolithen
- Jet-Phänomen in der Blase
- Phlebolithen in Ovarialvene
- asymmetrische Kontrastierung der Nieren
- ultrasound diagnosis of ureteral obstruction
- soft-tissue rim sign
- Konkrement im mittleren Ureter Sonographie
- native Computertomographie bei Ureterkonkrement
- Phlebolith vs. Ureterkonkrement
und weiter:
- Urolithiasis
- Nierensteine
- Minderperfusion der Niere
- rim sign in chronic hydronephrosis
- renal colic
- rim-sign (of ureteric calculi)
- soft tissue rim sign
- ultrasound diagnosis of ureteral obstruction: a middle ureter stone
- obstructing calculus in bifid ureter
- unenhanced helical CT imaging of an obstructing ureteric calculus
- Farbdoppler-Kometenartefakt
- Kometenschweif-Zeichen (Phlebolithen)
- Harnwegsinfekt
- multiple Füllungsdefekte im Ureter
- ureteric rupture


 Assoziationen und Differentialdiagnosen zu Harnleiterstein:
Assoziationen und Differentialdiagnosen zu Harnleiterstein: