intraossäres Lipom des Femurs





intraossäres Lipom des Femurs
intraossäres Lipom Radiopaedia • CC-by-nc-sa 3.0 • de
Intraosseous lipomas are rare benign lesions that account for about 0.1-2.5% of all bone tumors. It is, however, the most common lipogenic tumor in bone .
Epidemiology
It can present in an extremely wide age range (5-85 years) although the peak age at discovery is usually in the 4-5 decades of life. There may be a slight male predilection .
Clinical presentation
Pain is the leading symptom in the majority of cases, but more than 30% of bone lipomas are found incidentally on imaging studies done for other reasons .
Although intraosseous lipomas can be found essentially anywhere within the skeleton, the lower limb accounts for the majority of cases. When located in long bones, they tend to be found in the metaphysis :
- lower limb: 71%
- calcaneum: 32% (considered the most frequent calcaneal bone lesion)
- femur: 20% (especially the intertrochanteric region)
- tibia: 13%
- fibula: 6%
- upper limb: 7%
- skull and mandible: 7%
- spine and pelvis: 12%
- ribs: 2.5%
Pathology
Intraosseous lipomas are located almost exclusively within the medullary cavity, usually of long bones. They are composed of mature adipocytes without admixed hematopoietic tissue or bony trabeculae .
Radiographic features
Plain radiograph
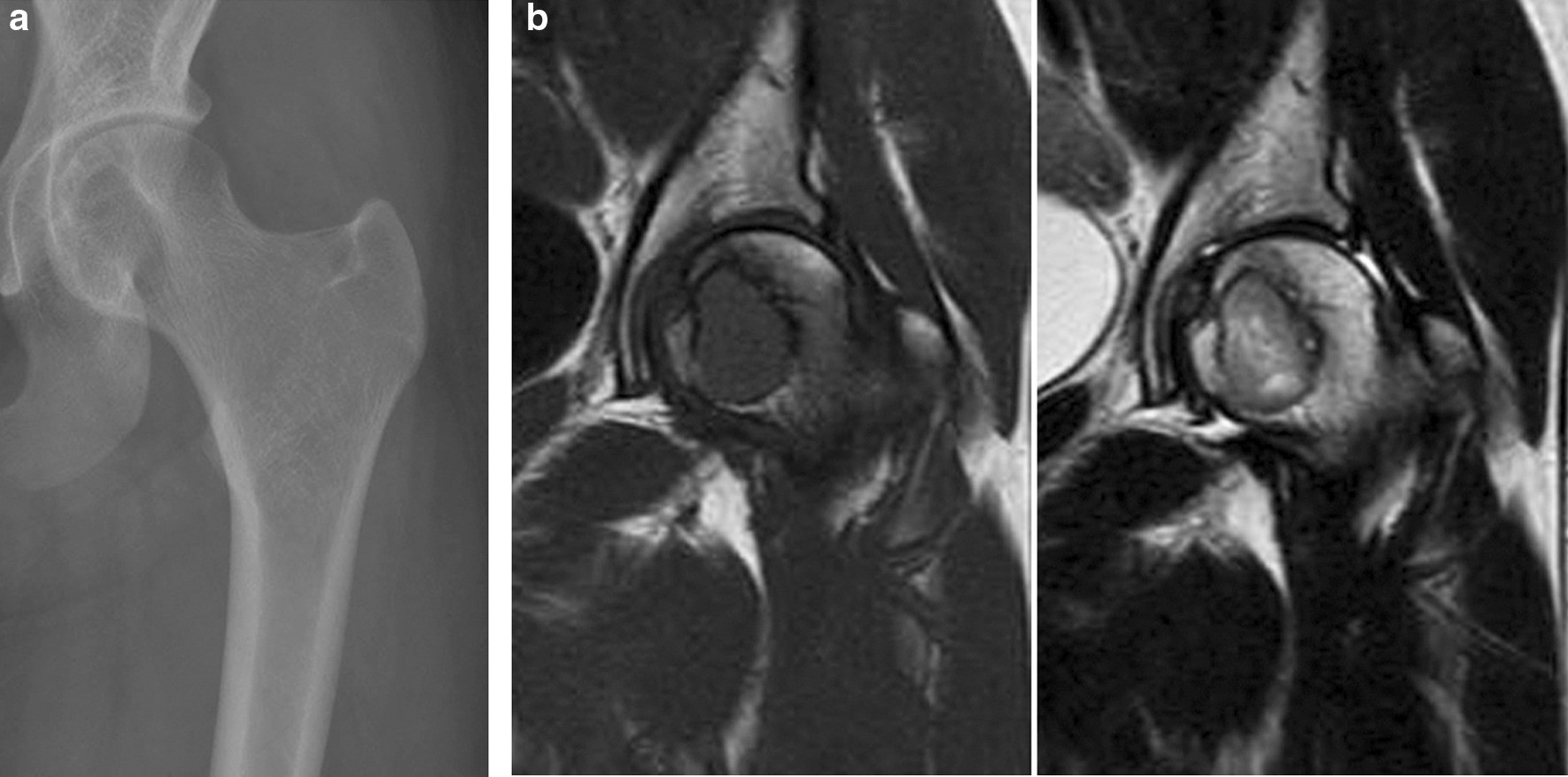
The radiographic appearance of intraosseous lipomas has a broad differential diagnosis, which includes many benign bone lesions. It may be typically seen as a rather benign-appearing osteolytic bone lesion with well-defined margins. Central calcification may develop creating the cockade sign.
CT/MRI
By CT attenuation or MRI signal characteristics, the differential diagnosis can be narrowed down to fat-containing lesions of the bone. The fatty components of intraosseous lipomas may display varying degrees of involution and necrosis. Based on these features, Milgram and co-workers proposed three categories:
- stage 1: sharply delineated, viable lipomas with homogeneous fat content
- stage 2: predominantly fatty lesions with central necroses, calcifications or ossifications
- stage 3: heterogeneous, fat-containing lesions with multiple necroses, cystic transformations, wall sclerosis and extensive calcifications or ossifications.
Stage 1
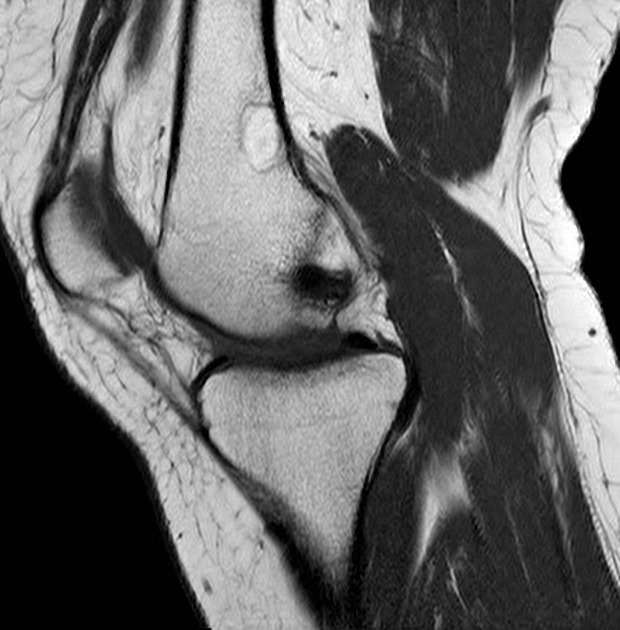
Accordingly, stage 1 lesions show homogeneous hyperintense fat signal on T1- and T2-weighted MR images that will be entirely suppressed by STIR or fat-saturated sequences. The trabecular cancellous bone pattern is typically absent within the lesion.
Stage 2
Stage 2 lesions show hypointense inclusions on T1-weighted images, which may appear hyperintense on fat-suppressed T2-weighted images (granulation tissue/necrosis) or hypointense (calcifications or ossifications).
Stage 3
In addition to the signal characteristics of stage 2 lesions, stage 3 lesions may contain fluid-equivalent cavities and signal-void bony septa, and are surrounded by thickened, signal-void rims of sclerotic bone. Although there are typically no signs of aggressive behavior, expansile intraosseous lipomas may outgrow the cortical border. This can be used to differentiate them from older bone infarcts, which may also develop cystic degeneration over time. Moreover, in intraosseous lipomas, T2-hyperintense granulation tissue of central necrosis is surrounded by viable fat tissue. Conversely, in bone infarcts, fat tissue in the center is surrounded by granulation tissue at the periphery. However, in cases with substantial secondary involution and necrosis, biopsy may be necessary to confirm the diagnosis .
Treatment and prognosis
Intraosseous lipomas that do not affect bone stability may be treated conservatively. Cases with imminent fractures are treated by curettage and bone grafting. There are no recurrences after surgical therapy. However, malignant transformations have been sporadically described .
Differential diagnosis
- in calcaneus: normal triangular lucency, in certain circumstances in plain film, a unicameral bone cyst (UBC) can also be considered
- in the proximal tibia: bone infarct
- in the proximal femur: liposclerosing myxofibrous tumor
Siehe auch:


 Assoziationen und Differentialdiagnosen zu intraossäres Lipom des Femurs:
Assoziationen und Differentialdiagnosen zu intraossäres Lipom des Femurs: