Juvenile aponeurotic fibroma
Calcifying aponeurotic fibromas are superficial benign potentially recurrent fibroblastic soft tissue tumors usually seen in the palms and soles of children and adolescents.
Terminology
Calcifying aponeurotic fibroma is also known as juvenile aponeurotic fibroma or just aponeurotic fibroma .
Epidemiology
Calcifying aponeurotic fibromas are rare. They usually occur in children and adolescents with a peak between the age of 5 and 15 years. Occasional cases in adults have been described. There is a male predilection .
Clinical presentation
The typical clinical manifestation of calcifying aponeurotic fibroma is a poorly demarcated painless soft tissue mass that is hard on palpation and might have been there for prolonged periods. Usually, it does not limit joint motion .
Complications
Joint contracture is a very infrequent complication .
Pathology
Calcifying aponeurotic fibromas are infiltrative fibroblastic proliferations usually composed of both fibromatosis-like and nodular calcifying components. They usually affect the volar fascia, aponeuroses and tendons of the distal extremities. There are also lesions that lack calcifications .
Etiology
The etiology of calcifying aponeurotic fibroma is unknown .
Location
Calcifying aponeurotic fibroma is frequently found in the following regions :
- palmar surfaces of hands and fingers
- plantar surfaces of feet and toes
- wrist and ankles (less common)
Unusual and rare locations are the following:
- proximal extremities
- trunk including the lumbosacral region
- head and neck
Macroscopic appearance
Macroscopically calcifying aponeurotic fibromas are ill-defined soft tissue masses with irregular contours, a grey-white color and a rough gritty consistency .
Microscopic appearance
The histological spectrum of calcifying aponeurotic fibromas includes the following features :
- an infiltrative moderately cellular fibromatosis-like component made up of uniform bland spindle cells
- hyalinized to chondroid calcified areas encircled by palisading epithelioid fibroblasts
- extension into the adjacent soft tissues
- possible entrapment of peripheral nerves and vessels
- low mitotic activity
- no cell atypia
Immunohistochemistry
Immunohistochemistry stains usually express smooth muscle actin (SMA), muscle-specific actin (MSA) CD99 and S100. β-catenin is typically negative .
Genetics
Calcifying aponeurotic fibromas are characterized by a fusion in the FN1-EGF gene.
Radiographic features
Reported imaging appearances of calcifying aponeurotic fibromas are limited in the literature. They are described as poorly demarcated non-specific soft tissue mass of the palmar or plantar surfaces with various degrees of calcifications .
Plain radiograph
Plain radiographs might reveal fine, stippled calcifications in the palms of hands and the soles of the feet, rarely associated with cortical erosion or scalloping .
Ultrasound
Calcifying aponeurotic fibromas have been described as lobulated lesions with hyperechoic foci and hypovascularity on color Doppler images .
CT
CT is the best modality for the characterization of the calcifications located in an otherwise non-specific soft tissue mass .
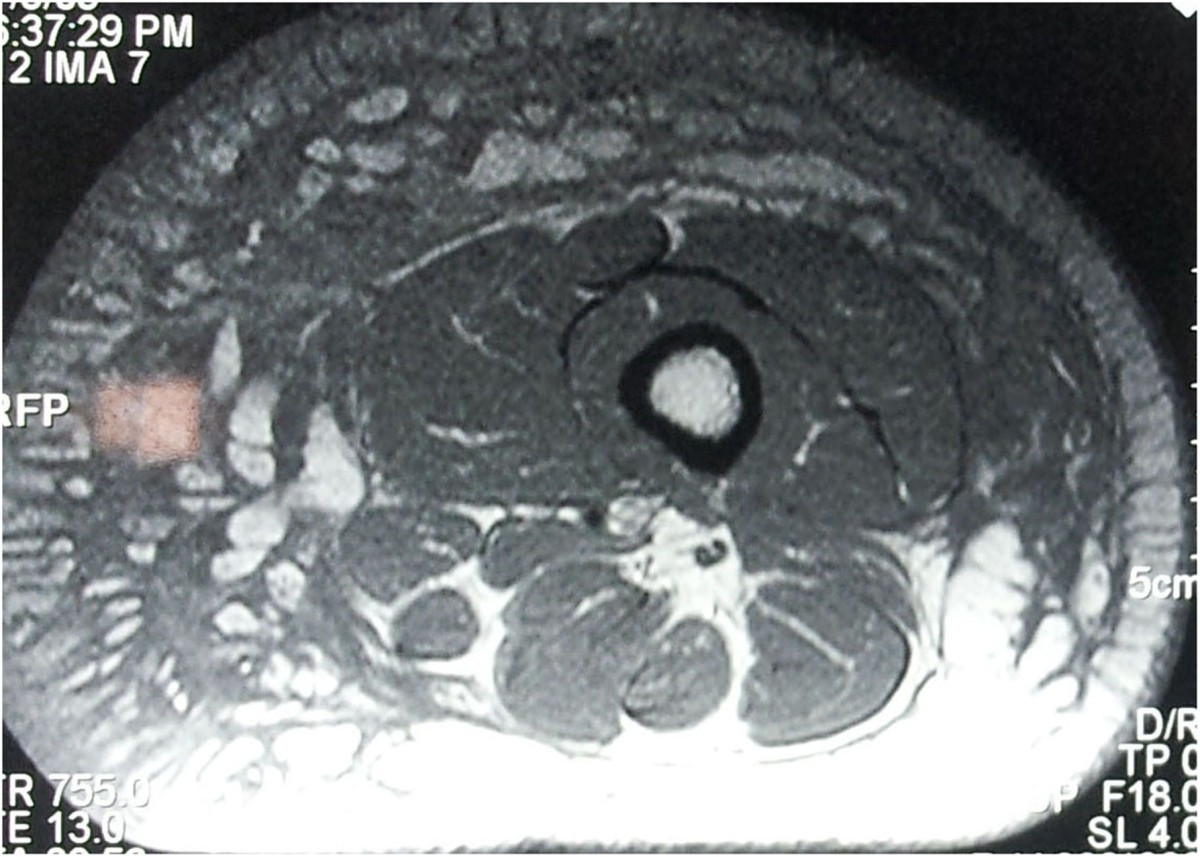
MRI
Imaging features are that of a superficial non-specific heterogenous round to oval soft tissue mass with small globular low signal intensity areas corresponding to calcifications .
Signal characteristics
- T1: low signal intensity compared to muscle
- T2: low signal intensity but slightly higher than muscle
- T1 C+ (Gd): intense heterogeneous enhancement
Radiology report
The radiological report should include a description of the following:
location and size of nodules
relation to adjacent bones
relation to adjacent tendons and muscular fascia
entrapment or relation to nerves and vessels
Treatment and prognosis
Surgical excision with preserving function preserving is usually done. Local recurrence is common and seen in up to 50% after primary excision. It seems to be more frequent in younger children and might occur even after several years. Multiple recurrences are rare due to limited growth potential .
History and etymology
The entity was initially described in 1953 by LE Keasbey as juvenile aponeurotic fibroma .
Differential diagnosis
Conditions which can mimic the appearance of inclusion body fibromatosis include :


 Assoziationen und Differentialdiagnosen zu Juvenile aponeurotic fibroma:
Assoziationen und Differentialdiagnosen zu Juvenile aponeurotic fibroma: