Oligodendrogliom










Oligodendrogliomas are intracranial tumors that account for 5-25% of all gliomas and 5-10% of all primary intracranial neoplasms.
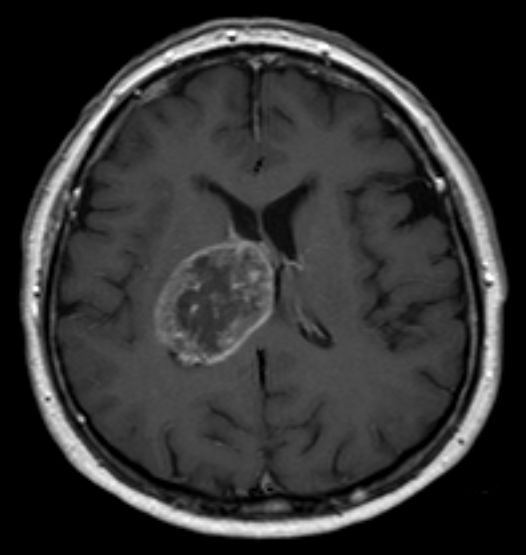
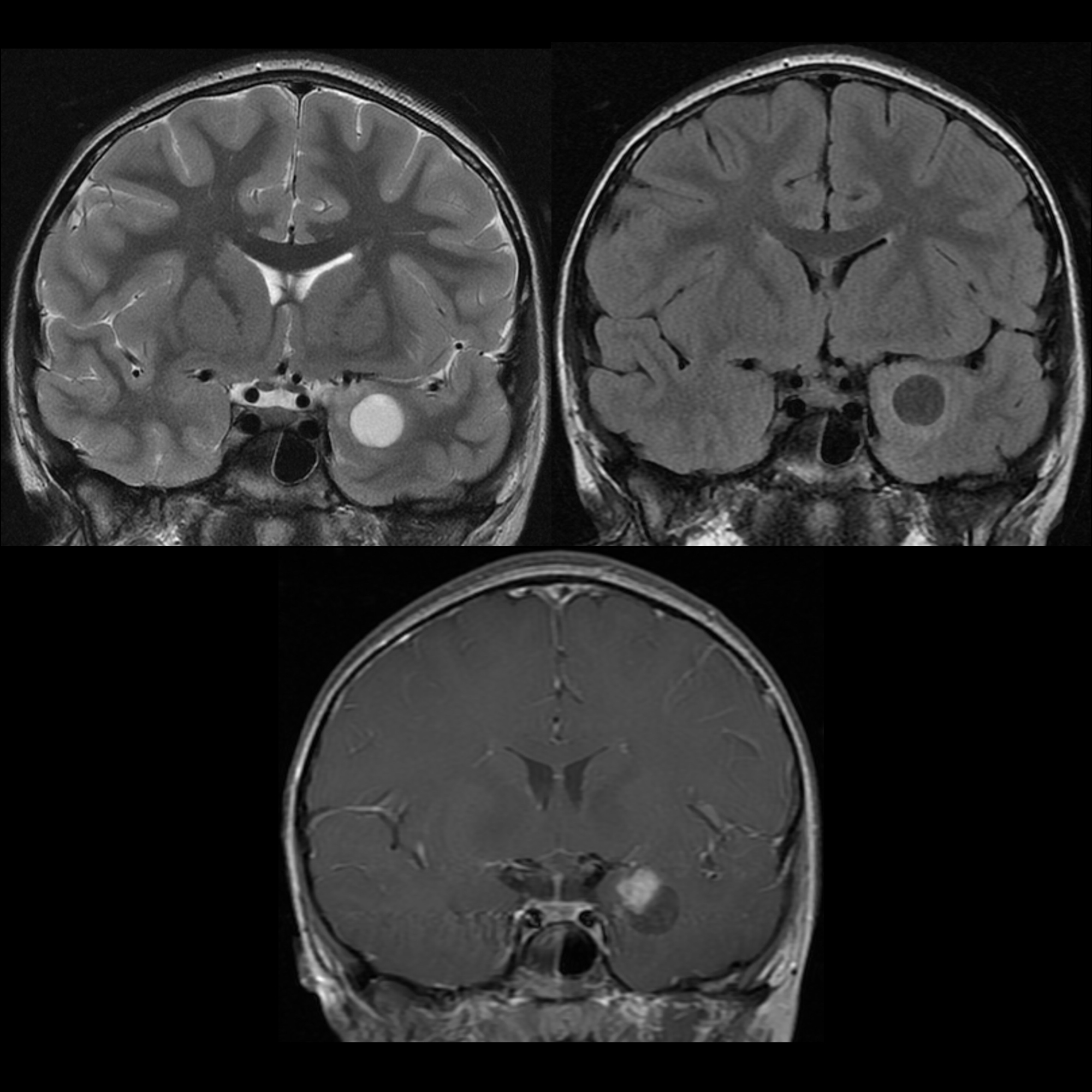
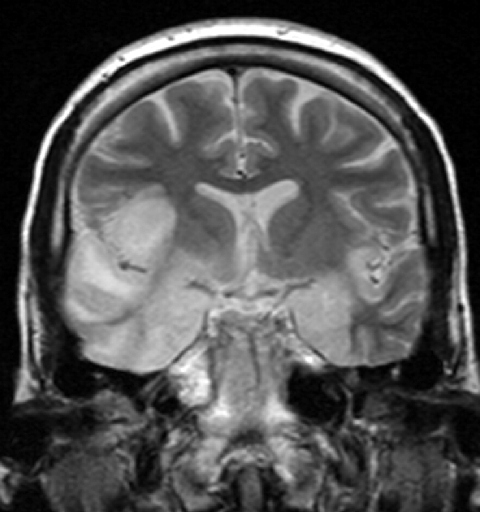
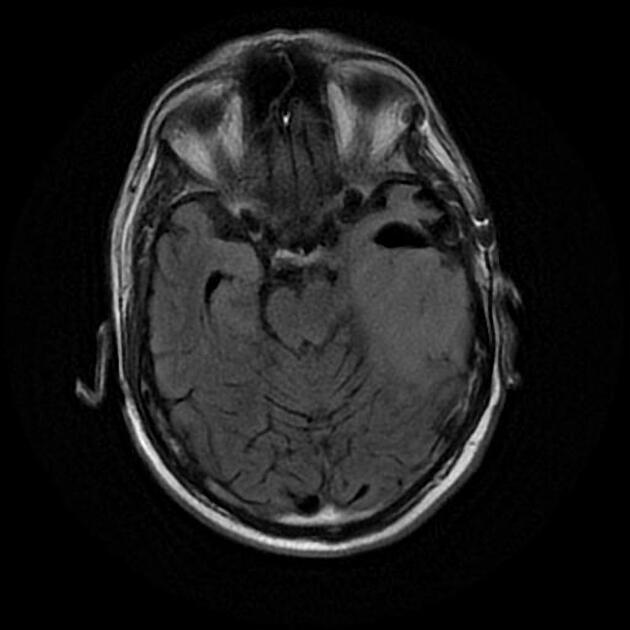
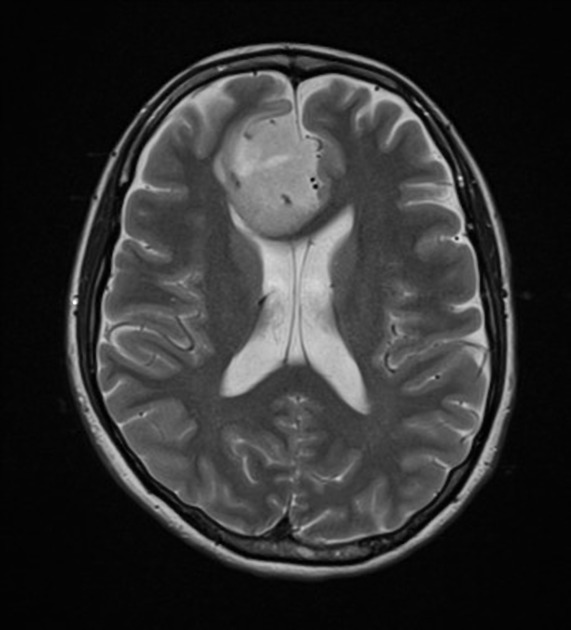
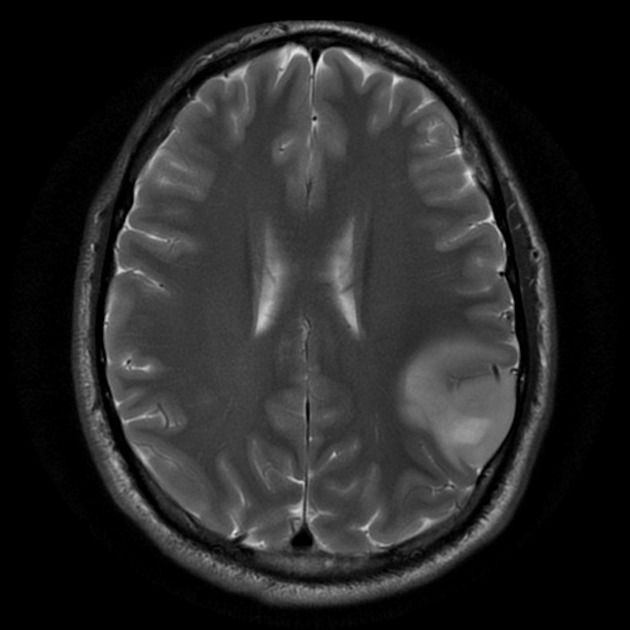
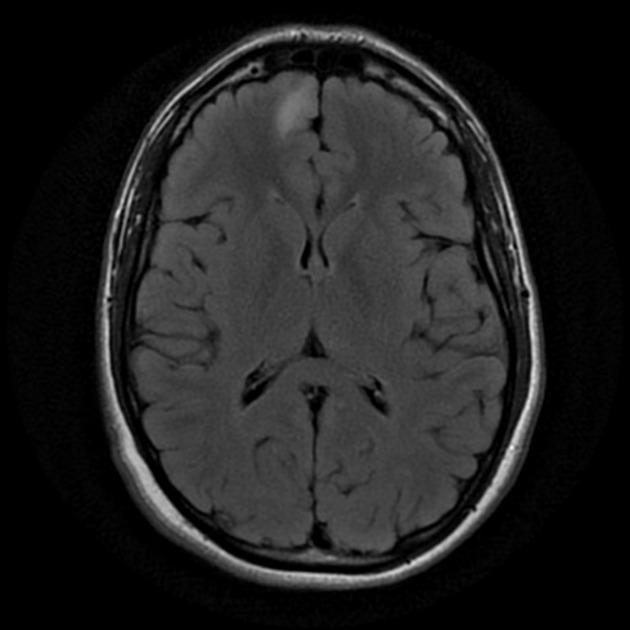
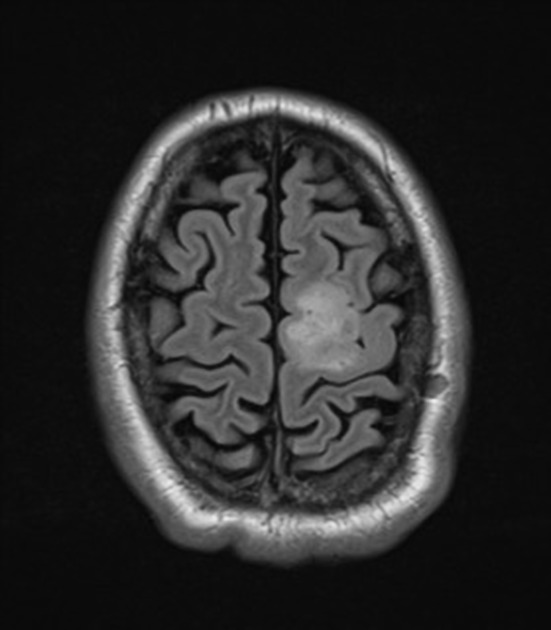
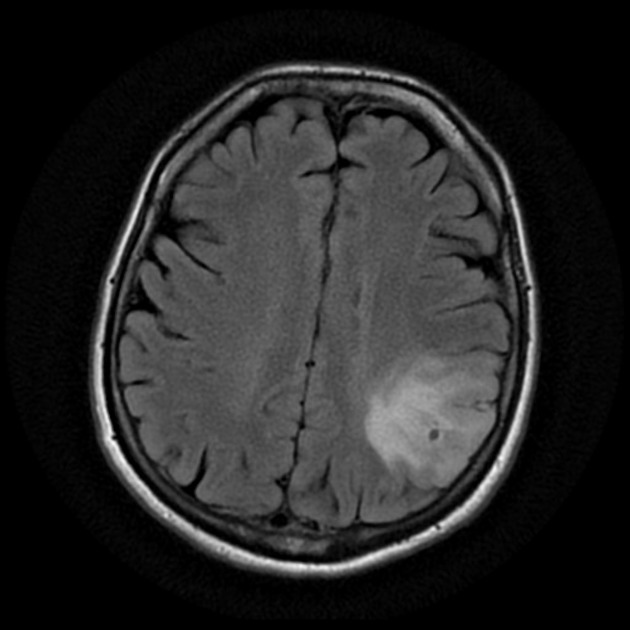
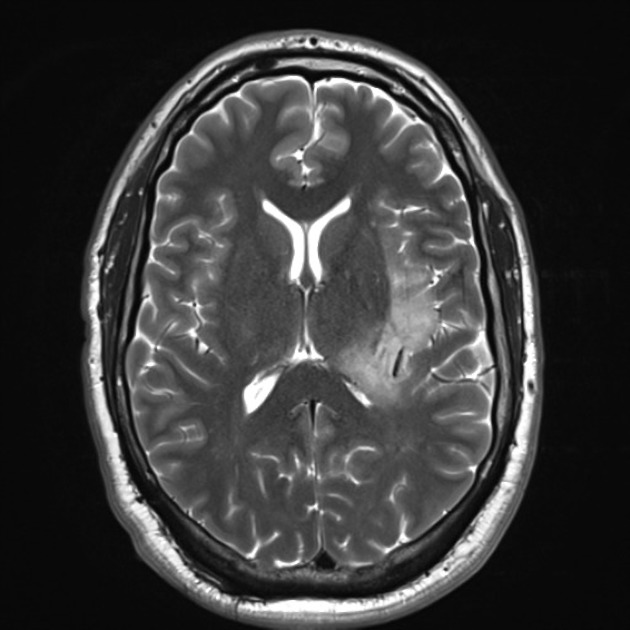
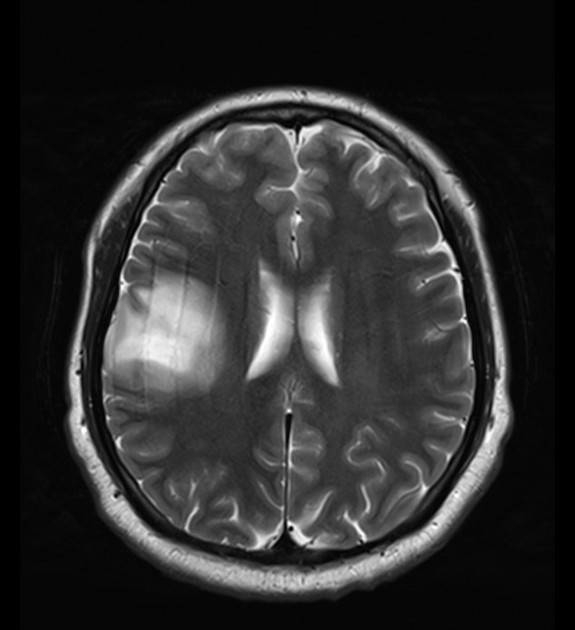
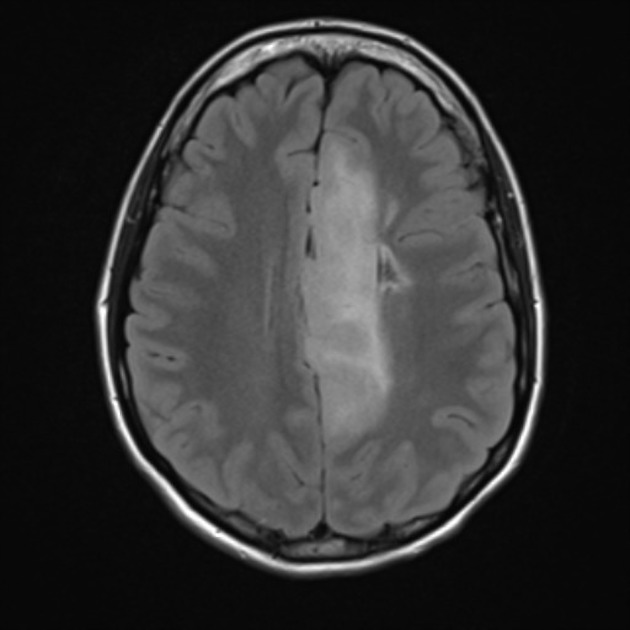
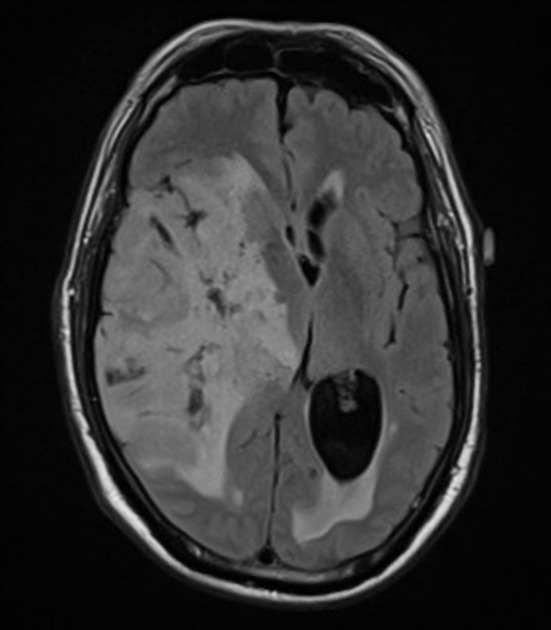
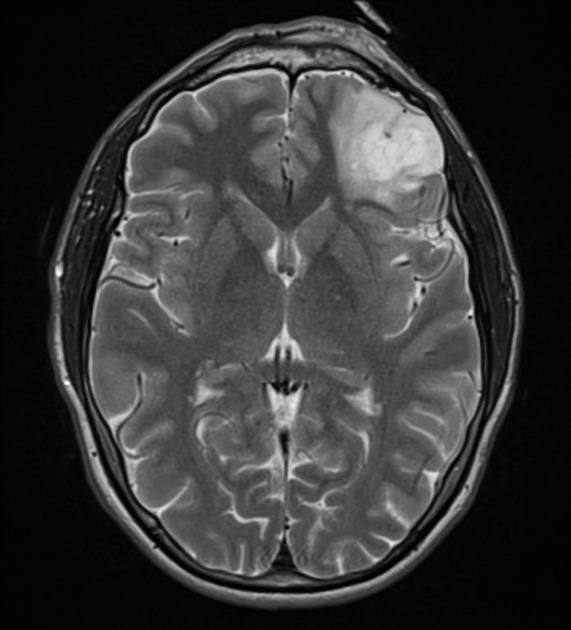
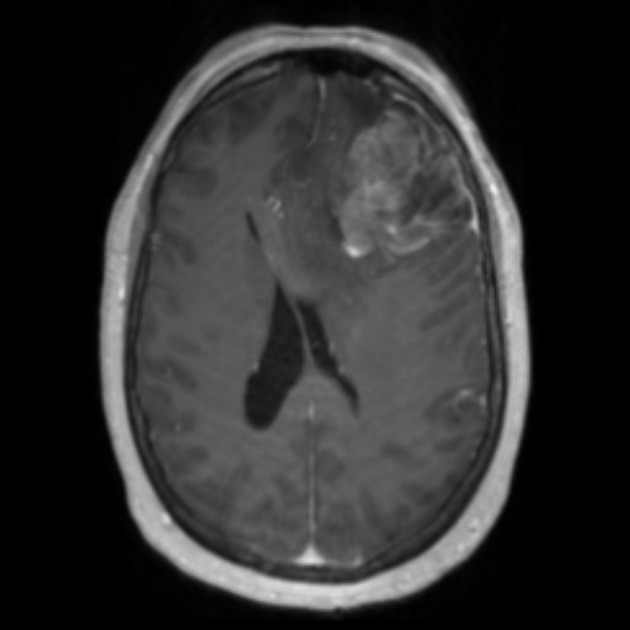
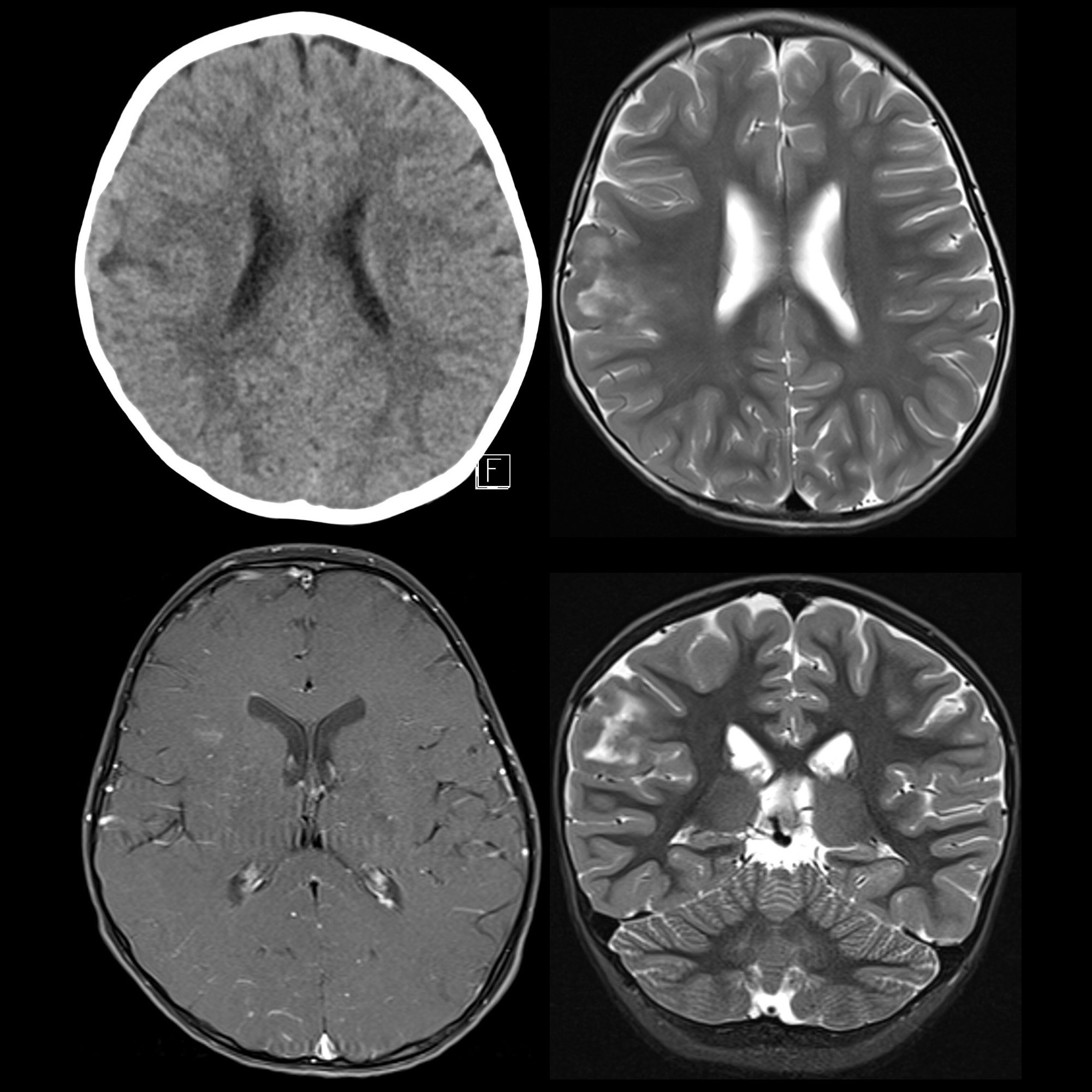
On imaging, oligodendrogliomas commonly present as masses involving the cortex or subcortical white matter, with low attenuation on CT, hypointense compared to grey matter on T1 and hyperintense compared to grey matter on T2-weighted MRI images. The attenuation or signal can be eventually heterogeneous due to calcification, cystic degeneration and hemorrhage.
Terminology
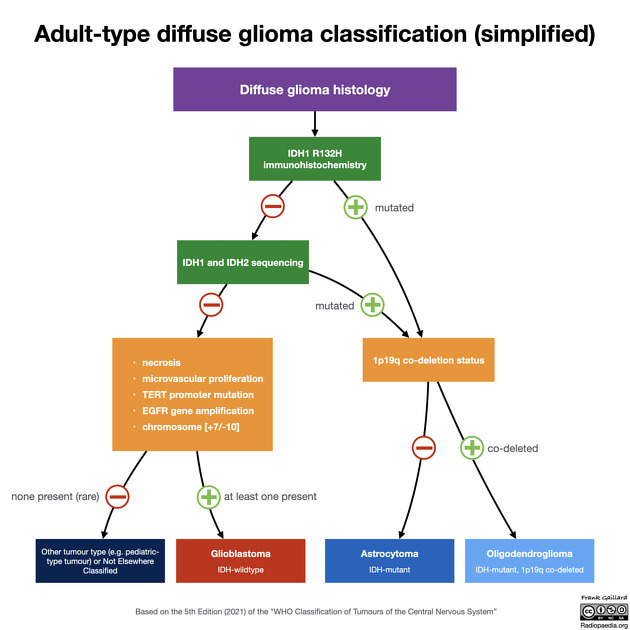
Historically, oligodendrogliomas have been defined on histological grounds. As of 2016, however, with the update to the WHO classification of CNS tumors the diagnosis of oligodendroglioma is made by identifying a diffuse infiltrating glioma with IDH mutation and 1p19q codeletion . This is a very significant change, as the tumors previously diagnosed as oligodendrogliomas on the grounds of histology, and those currently diagnosed on the basis of the molecular markers are not identical, with different imaging features. As such it is essential when reading about gliomas to ascertain which definition is being used. As a general rule, anything written before 2016 will use histology alone.
The reliance on molecular markers is, however, not foolproof. Sometimes molecular markers are unavailable (in many countries or regional centers) or sometimes equivocal. In such instances, the diagnosis reverts to histological features alone, and are termed Not-Otherwise-Specified (NOS) . Clearly, as the two groups are not the same, this is creating problems when interpreting the literature.
The WHO classification of CNS tumors, therefore, recognizes four diagnoses related to oligodendrogliomas :
In addition, oligoastrocytomas are also recognized but discussed separately.
Epidemiology
Oligodendroglioma is considered the third most common glioma accounting for 2%–5% of primary brain tumors and 5%–18% of all glial neoplasms .
Oligodendrogliomas are usually tumors of middle-aged adults, occurring most commonly in the 4 and 5decades of life. They are rare in children . There is a slight male predilection (M:F 1.3:1) .
Clinical presentation
Due to frequent cortical involvement, they most commonly (two-thirds of patients) present with seizures . Otherwise, clinical presentation is non-specific with symptoms related to increased intracranial pressure and focal neurological deficits being common.
Pathology
Location
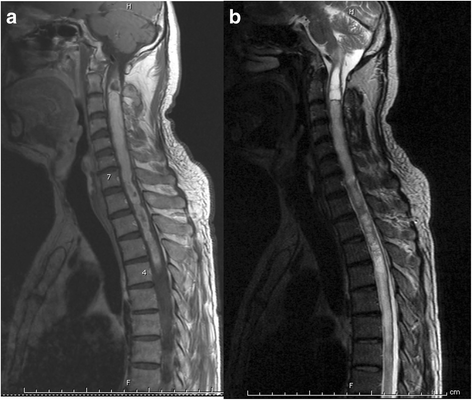
The vast majority of oligodendrogliomas arise in the cerebral hemispheres, with brainstem, cerebellum and spinal cord being distinctly uncommon .
Gross appearance
Historically, oligodendrogliomas were considered well-circumscribed, gelatinous, grey masses, and this remains true of histologically defined oligodendrogliomas NOS. IDH-mutant and 1p19q co-deleted oligodendrogliomas, however, appear to be a different group of tumors and recent studies suggest that in fact they have poorly defined borders .
Oligodendrogliomas are often calcified (70-90% of histological oligodendrogliomas: one of the most frequently calcifying tumors) and also frequently demonstrate focal hemorrhage . Cystic change is also quite common. Slow growing cortical tumors can often expand a gyrus and eventually remodel the skull.
Microscopic appearance and classification
It is essential to appreciate that as of the 2016 update to the WHO classification of CNS tumors, to formally make the diagnosis of oligodendroglioma, a tumor must be shown to have IDH-mutation and 1p19q co-deletion (see Terminology section above).
Oligodendroglioma (WHO grade II)
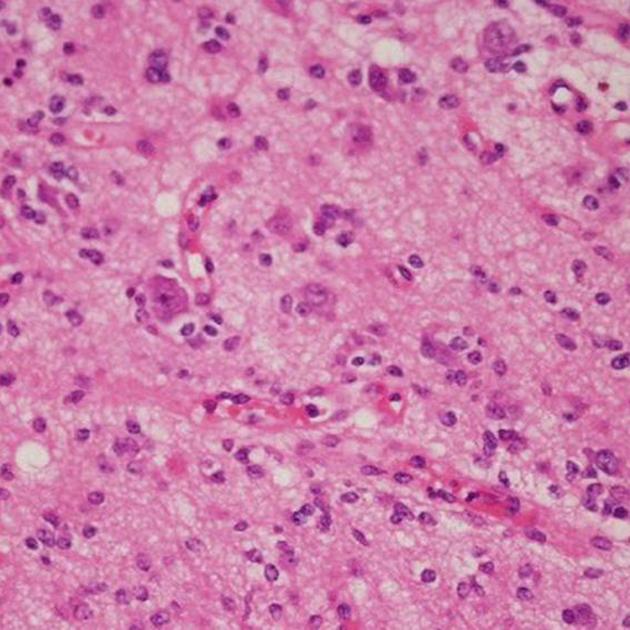
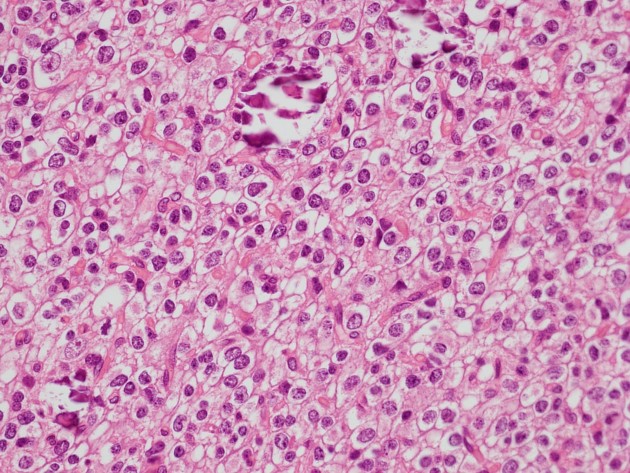
Neoplastic oligodendrocytes appear as regular cells with spherical nuclei containing finely granular chromatin surrounded by a halo of cytoplasm "fried egg" appearance under the light microscope. Typically contains a delicate network of anastomosing capillaries giving it a so-called "chicken wire" appearance . These tumors are slowly growing.
Anaplastic oligodendroglioma (WHO grade III)
Anaplastic oligodendrogliomas (discussed separately) demonstrate increased cellular density, increased mitotic activity, microvascular proliferation and necrosis. Nuclear anaplasia is also common.
Importantly, and unlike astrocytomas, oligodendrogliomas with necrosis and microvascular proliferation are considered only WHO grade III anaplastic oligodendrogliomas and not WHO grade IV glioblastomas .
Oligoastrocytoma
Oligoastrocytomas (discussed separately) are tumors of mixed oligodendroglioma and astrocytoma cell populations, that have historically been variably reported depending on local practice. As of the 2016 update to the WHO classification of CNS tumors, to make the diagnosis genomic evidence of both astrocytic and oligodendroglial components will be required to make the diagnosis, and as such, they are likely to become rare .
Radiographic features
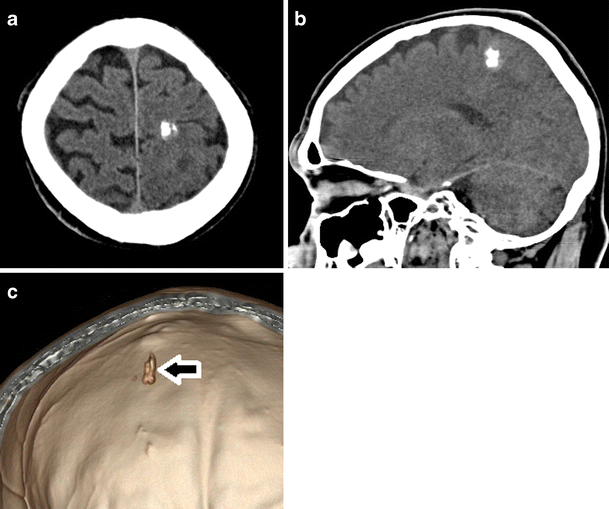
CT
Non-contrast CT
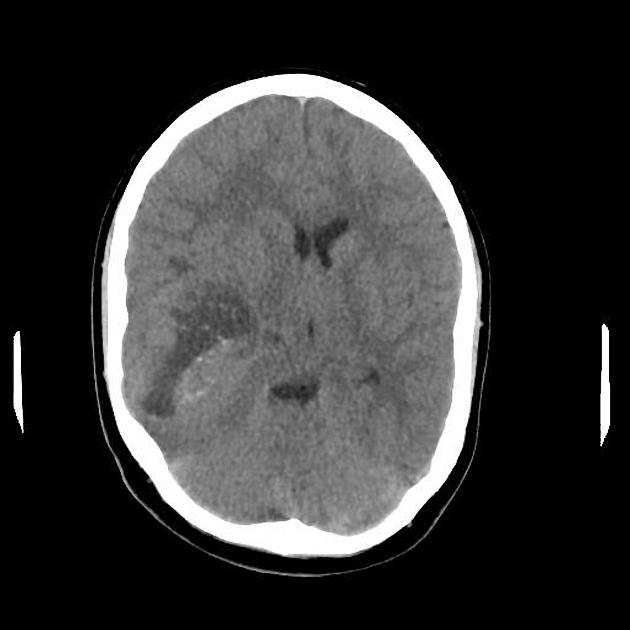
Tumors are of mixed density (hypodense to isodense). High-attenuation areas within the tumor are likely from calcification (70-90% of oligodendrogliomas are calcified) or, less commonly, hemorrhage. Calcification can be located centrally, peripherally or can be ribbon-like . The overlying skull may show pressure remodeling.
Post-contrast CT
Approximately 50% of oligodendrogliomas enhance: the degree of enhancement is extremely variable, ranging from no enhancement to strikingly vivid enhancement.
MRI
The MRI appearances also vary depending on whether a histological diagnosis or a molecular definition is used.
Oligodendrogliomas NOS, or those tumors that histologically show oligodendroglial features but are 1p/19q intact show more homogeneous signal on T1 and T2 images and have sharper borders than 'true' oligodendroglioma, those with 1p/19q co-deletion . In fact, a well-circumscribed homogeneously hypoattenuating non-calcified cortical tumor is probably predictive of not having 1p19q codeletion .
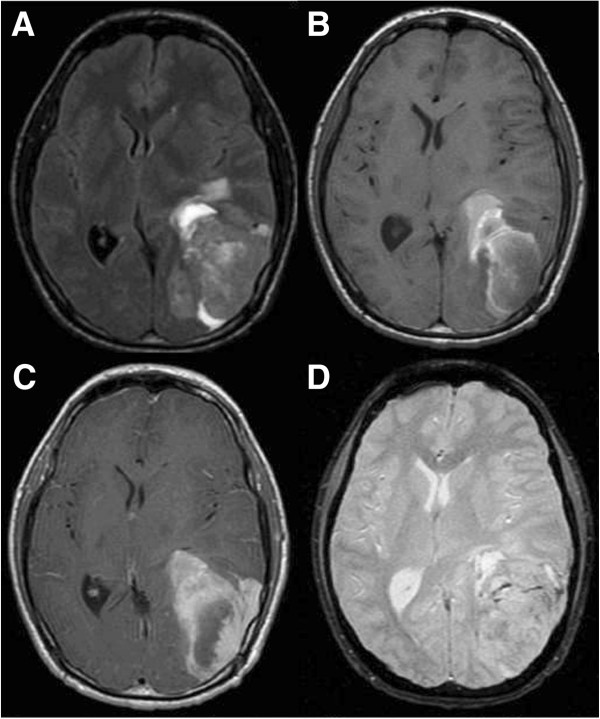
Calcification and hemorrhage are difficult to distinguish on MR, appearing as areas of signal loss on T2* sequences, but phase component of SWI may help. Peritumoral vasogenic edema is minimal.
- T1: typically hypointense
- T2: typically hyperintense (except calcified areas)
- T2*: calcium can be seen as areas of "blooming"
- T1 C+ (Gd): contrast enhancement is common but it is not a reliable indicator of tumor grade, with only 50% of oligodendrogliomas enhancing to a variable degree, and usually heterogeneously
- DWI
- typically no diffusion restriction
- DWI can be used to help differentiate oligodendrogliomas (generally lower grade) from astrocytomas (generally higher grade); astrocytomas have higher ADC values probably because of their lower cellularity and greater hyaluronan proportion .
- MR perfusion (PWI): increased vascularity "chicken wire" network of vascularity results in elevated relative cerebral blood volume (rCBV) of grade II vs grade III on PWI; PWI has a sensitivity of 95% and PPV or 87% for distinguishing grade II from grade III oligodendrogliomas; a threshold of 1.75, rCBV above this threshold demonstrates more rapid tumor progression
PET
C-Methionine studies can be used to differentiate oligodendrogliomas from anaplastic oligodendrogliomas. FDG uptake of oligodendrogliomas is similar to normal white matter. FDG uptake of anaplastic oligodendrogliomas is similar to normal grey matter.
Treatment and prognosis
As mentioned earlier response to radiochemotherapy and hence prognosis depends significantly on the presence or absence of 1p19q gene deletion .
Treatment is surgical, with adjuvant radiotherapy and chemotherapy. Although they are macroscopically well delineated, infiltration is present at their margins and local recurrence is common.
Survival statistics are primarily available for histologically defined oligodendrogliomas and tend to demonstrate 10 year-survival of approximately 50% .
Differential diagnosis
General imaging differential considerations include:


 Assoziationen und Differentialdiagnosen zu Oligodendrogliom:
Assoziationen und Differentialdiagnosen zu Oligodendrogliom: