pontine hemorrhage
Pontine hemorrhage, a form of intracranial hemorrhage, is most commonly due to long standing poorly-controlled chronic hypertension. It carries a very poor prognosis.
Epidemiology
Primary pontine hemorrhage accounts for ~7.5% (range 5-10%) of hemorrhagic strokes and has an incidence of ~3 per 100,000 people .
Clinical presentation
Patients present with sudden and precipitous neurological deficits. Depending on the speed at which the hematoma enlarges and the exact location, presentation may include :
- decreased level of consciousness (most common)
- long tract signs including tetraparesis
- cranial nerve palsies
- seizures
- Cheyne-Stokes respiration
Pathology
As is the case with penetrating arteries into the basal ganglia, the penetrating arteries from the basilar artery extending into the pons are subject to lipohyalinosis as a result of poorly-controlled hypertension . This renders the vessel wall prone to rupture. The larger paramedian perforators are more commonly the culprit vessels .
Hemorrhage into the pons can of course also be secondary to underlying lesions including:
- vascular malformations
- tumors
- neuroepithelial (primary) brain tumors
- metastases
- central downward transtentorial herniation (Duret hemorrhages)
- supratentorial surgery (remote hemorrhage)
Radiographic features
CT
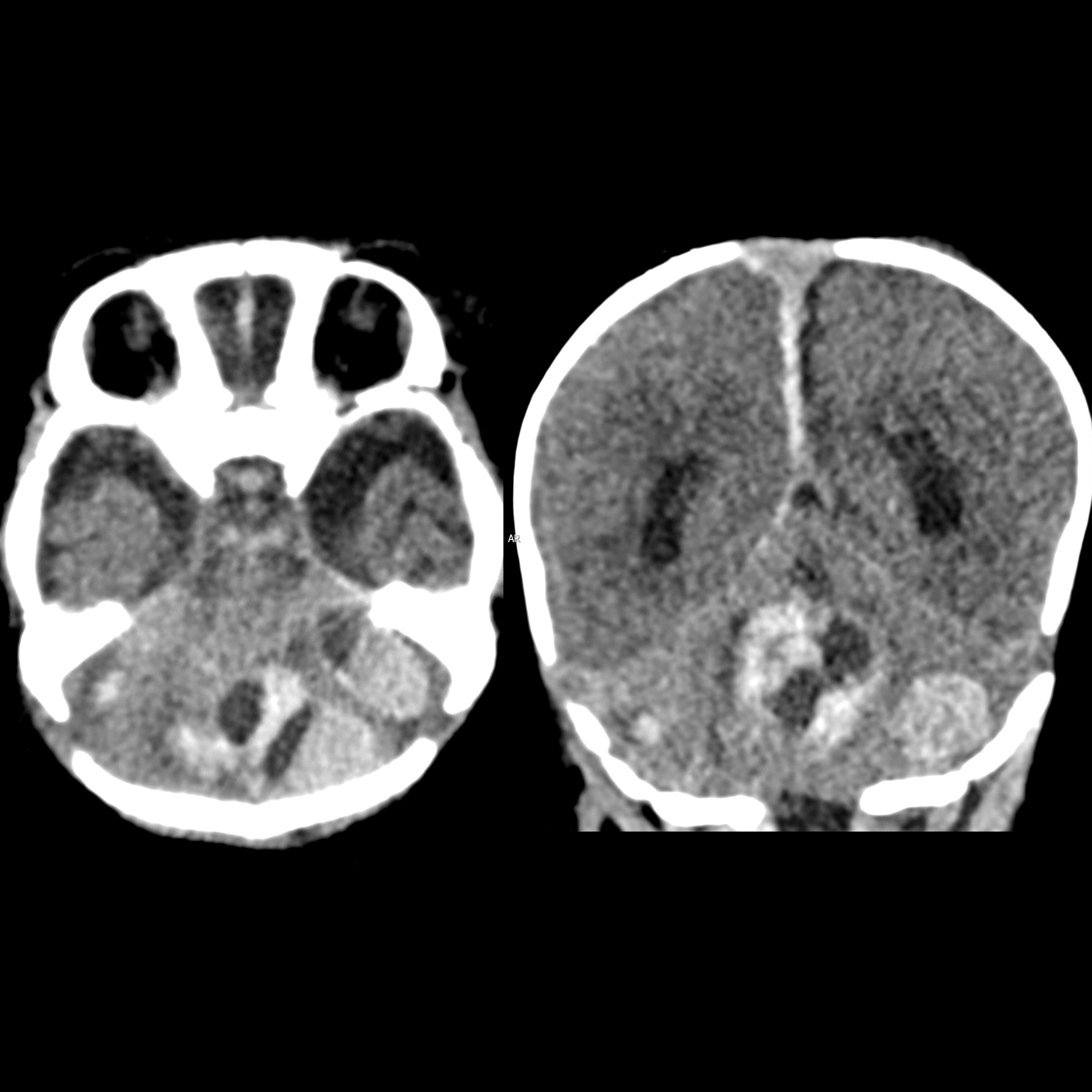
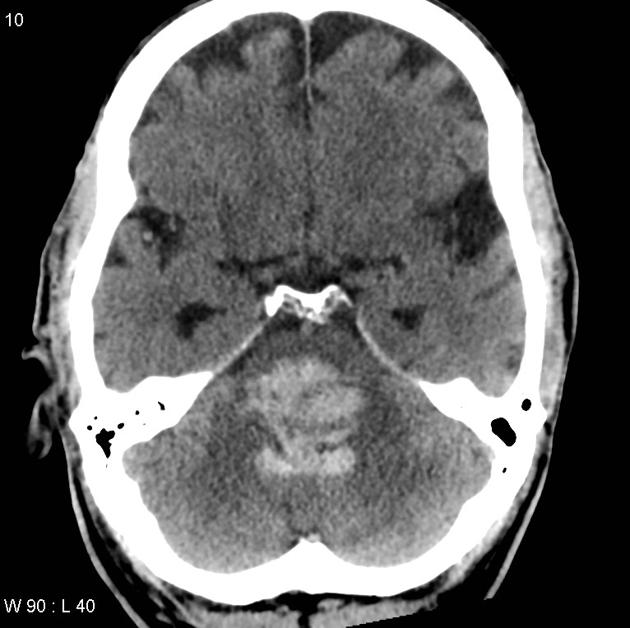
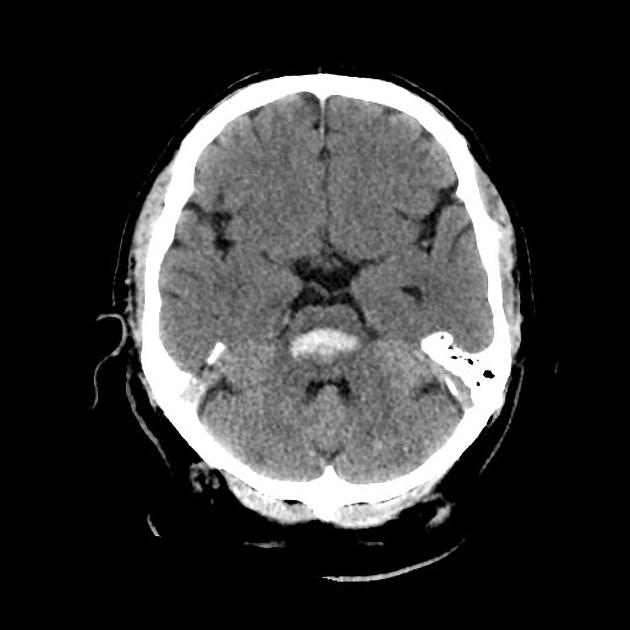
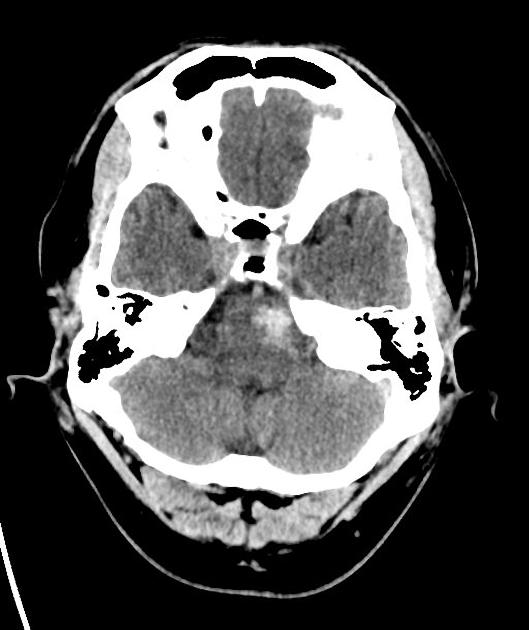
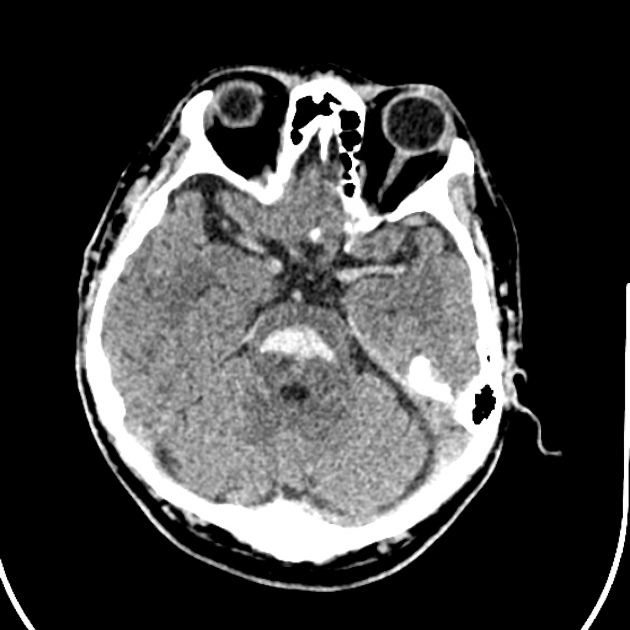
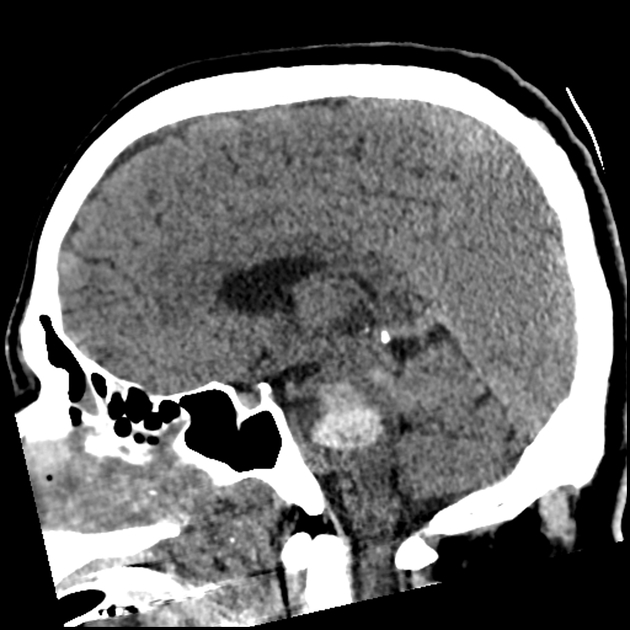
CT of the brain is usually the first, and often the only, investigation obtained upon presentation. Features typical of an acute intraparenchymal hemorrhage are noted, usually located centrally within the pons (on account of the larger paramedian perforators usually being the site of bleeding).
The hematoma more frequently extends in a rostrocaudal direction along the traversing long tracts rather than laterally into the middle cerebellar peduncles. Usually the hematoma does not extend beyond the pontomedullary junction inferiorly and the inferior midbrain superiorly .
These hematomas frequently rupture into the 4 ventricle .
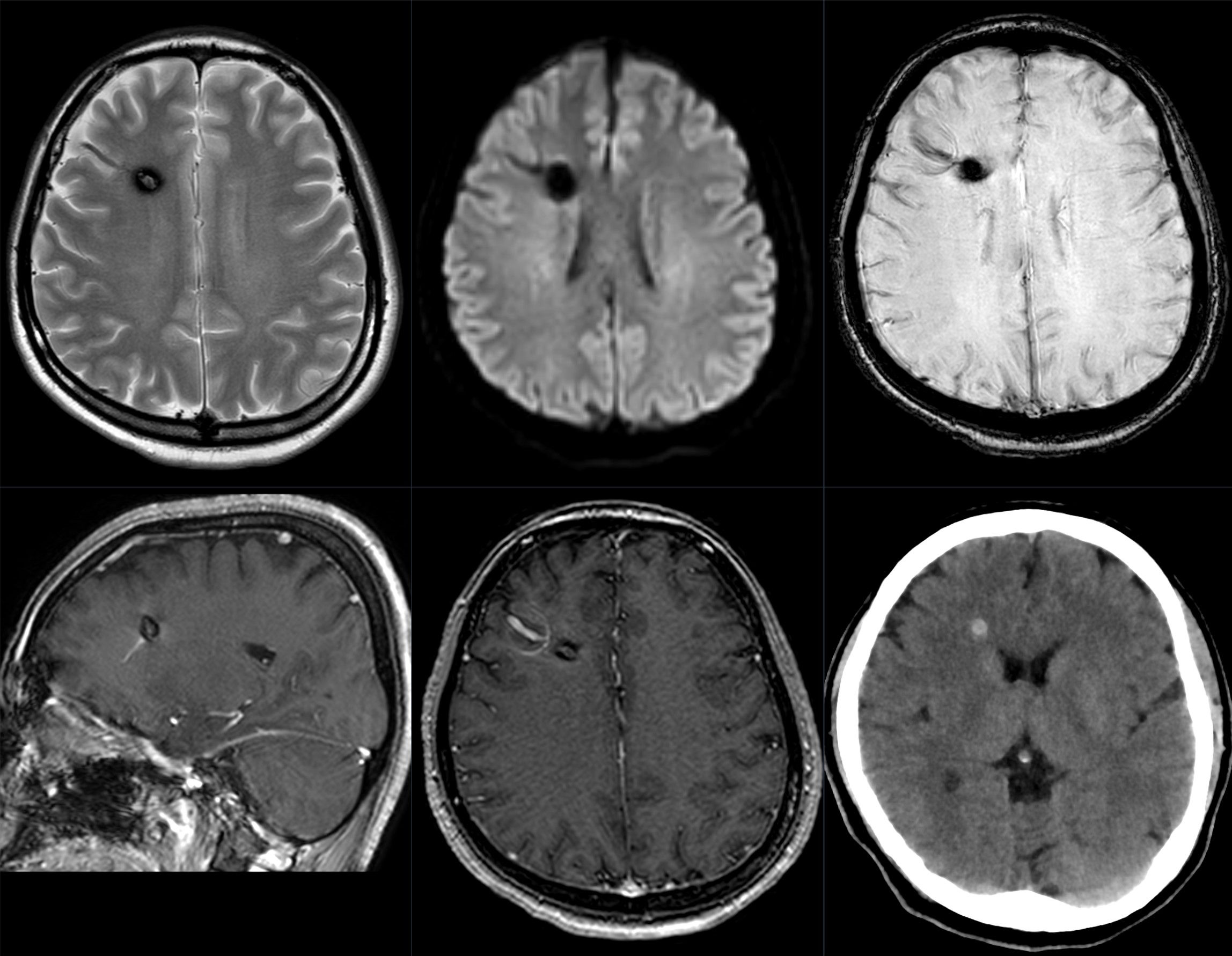
In patients who have small volume bleeds and who are thought to possibly have an underlying lesion, MRI may be of use (e.g. identification of a vascular malformation).
Treatment and prognosis
Pontine hemorrhages have a poor prognosis, with large bleeds being almost universally fatal. Open surgical evacuation of the clot is usually not performed, although stereotactic clot aspiration has been advocated by some .
In smaller hemorrhages, medical management and treatment of hydrocephalus with extraventricular drains may be life saving, however, often with significant residual neurological deficits.
Overall mortality ranges between 30% and 90% , with the overall volume of the bleed and initial GCS being related to outcome .
Differential diagnosis
The main differential is between a primary pontine hemorrhage and hemorrhages resulting from underlying lesions (see above). Usually patients present suddenly with severe impairment and the diagnosis is not difficult to make.
In patients where the presentation is not known (e.g. in the exam setting) it is worth considering:
- unruptured/asymptomatic vascular malformations
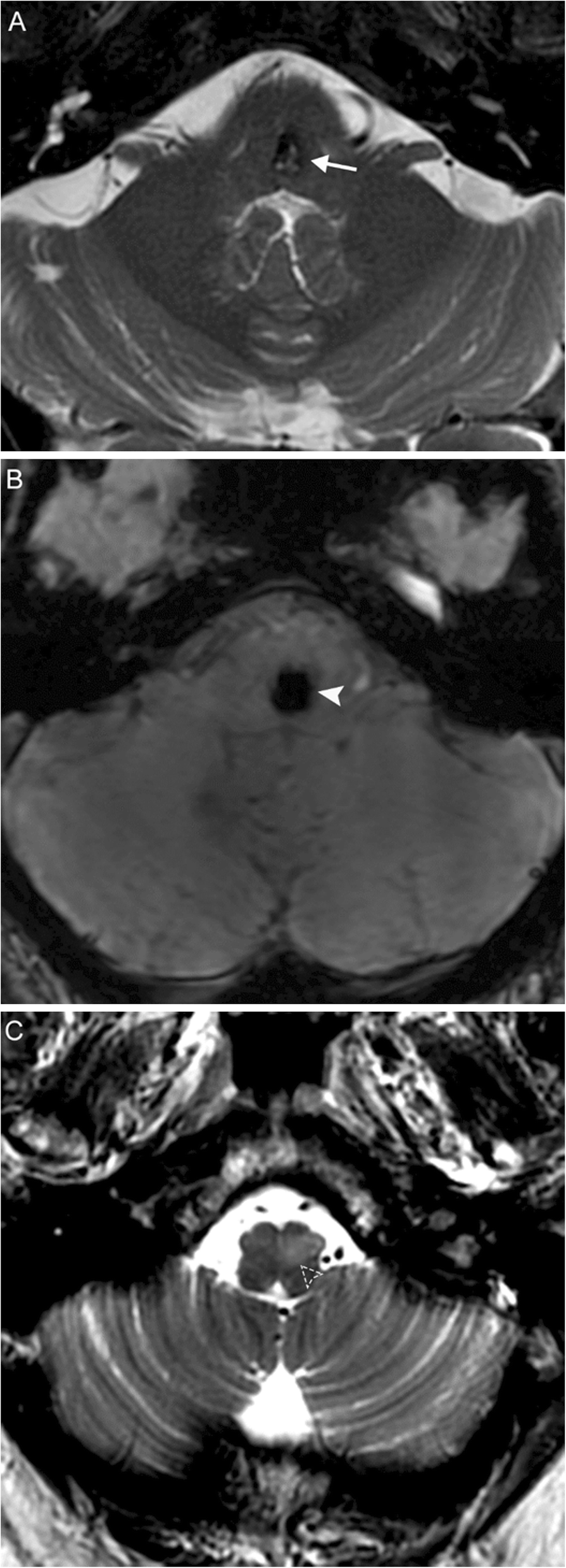
- asymptomatic cavernous malformations (these can periodically have small bleeds resulting in repeated symptoms)
- arteriovenous malformation
- usually little if any mass effect
- serpentine irregular density isodense to intravascular blood elsewhere
- developmental venous anomaly
- linear, no mass effect
- density isodense to intravascular blood elsewhere
- hemorrhagic metastases
Siehe auch:
- Developmental Venous Anomaly
- Arteriovenöse Malformation
- pontine kapilläre Teleangiektasie
- Kleinhirnblutung
- Kavernom
- Verkalkung Pons
- Hypertrophe Degeneration der Olive
- vaskuläre Anomalien im Pons
- hämorrhagischer Ponsinfarkt
- eingeblutete Metastasen
und weiter:


 Assoziationen und Differentialdiagnosen zu Ponsblutung:
Assoziationen und Differentialdiagnosen zu Ponsblutung: