radial head dislocation



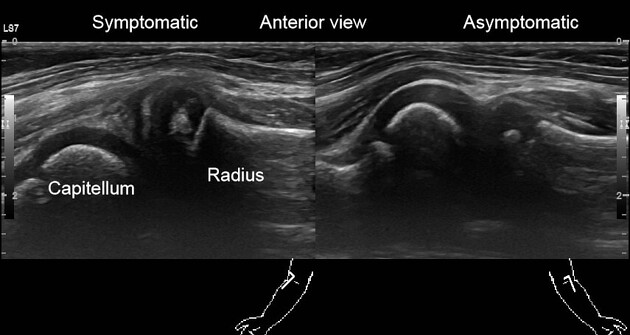











Radial head dislocation occurs when the radial head is displaced from its normal articulation with the ulna and the humerus.
The dislocation may be acquired or congenital (see the separate article on congenital radial head dislocation). Additionally, radial head dislocation should be distinguished from a 'pulled elbow' with represents radial head subluxation and reduces spontaneously or with rapid supination.
Epidemiology
Radial head dislocation is usually seen in infancy or childhood where it is usually an isolated injury.
Clinical presentation
Children who present with dislocation of the radial head usually demonstrate an unwillingness to use the arm. The history is not usually particularly helpful in distinguishing this injury from any other although a fall on an outstretched arm is not uncommon.
Pathology
The radius and ulna are bound to each other at both ends at the aptly-named proximal and distal radioulnar joints. Akin to the mandible and pelvis, it is difficult to disrupt one side of a ring without also disrupting the other. Thus, it is important to ensure that radial head dislocation is truly isolated and not associated with an ulna fracture (the Monteggia fracture-dislocation).
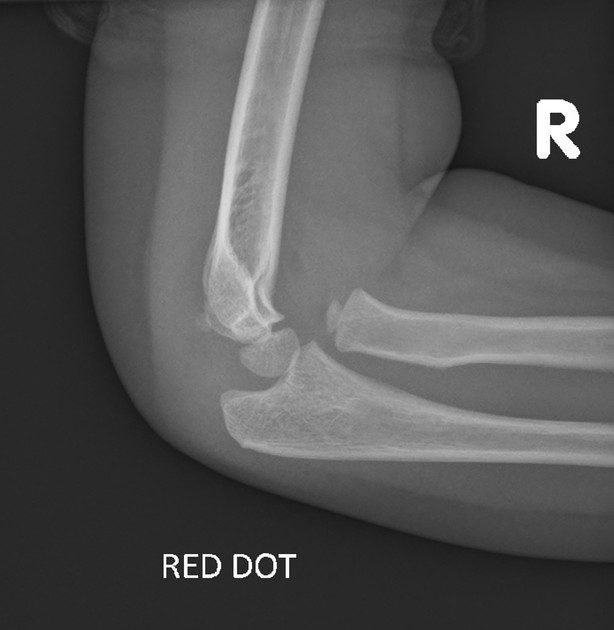
Plastic deformation of bones is common in pediatric patients. Therefore, rather than radial head dislocation being associated with an transverse ulna fracture, the ulna develops a bowing fracture instead. Monteggia fracture-dislocation is uncommon in children, but it is by no means rare .
Dislocation of the radial head is also seen in individuals with neuromuscular disorders and contractures, e.g. cerebral palsy and brachial plexus injuries .
Radiographic features
Plain radiograph
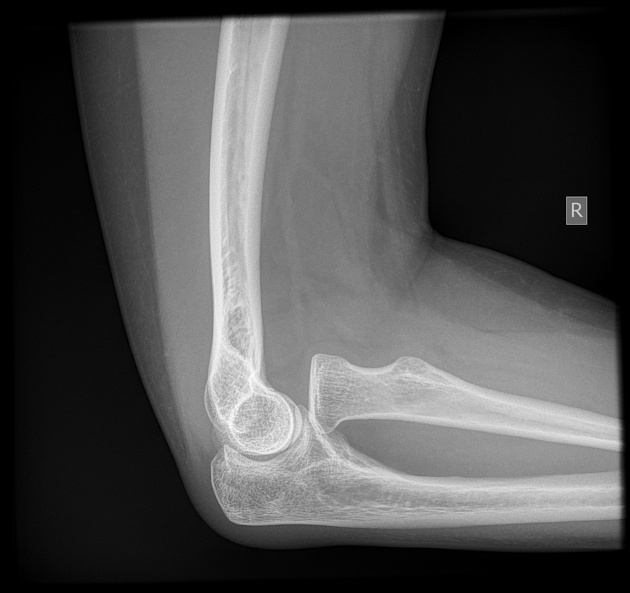
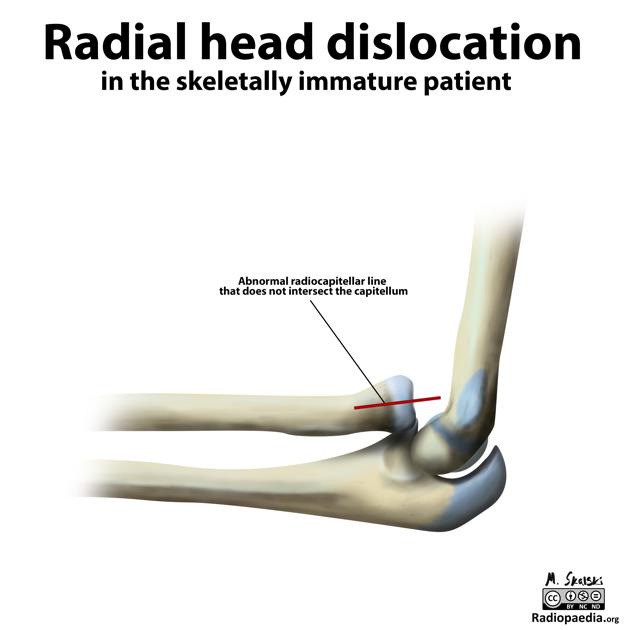
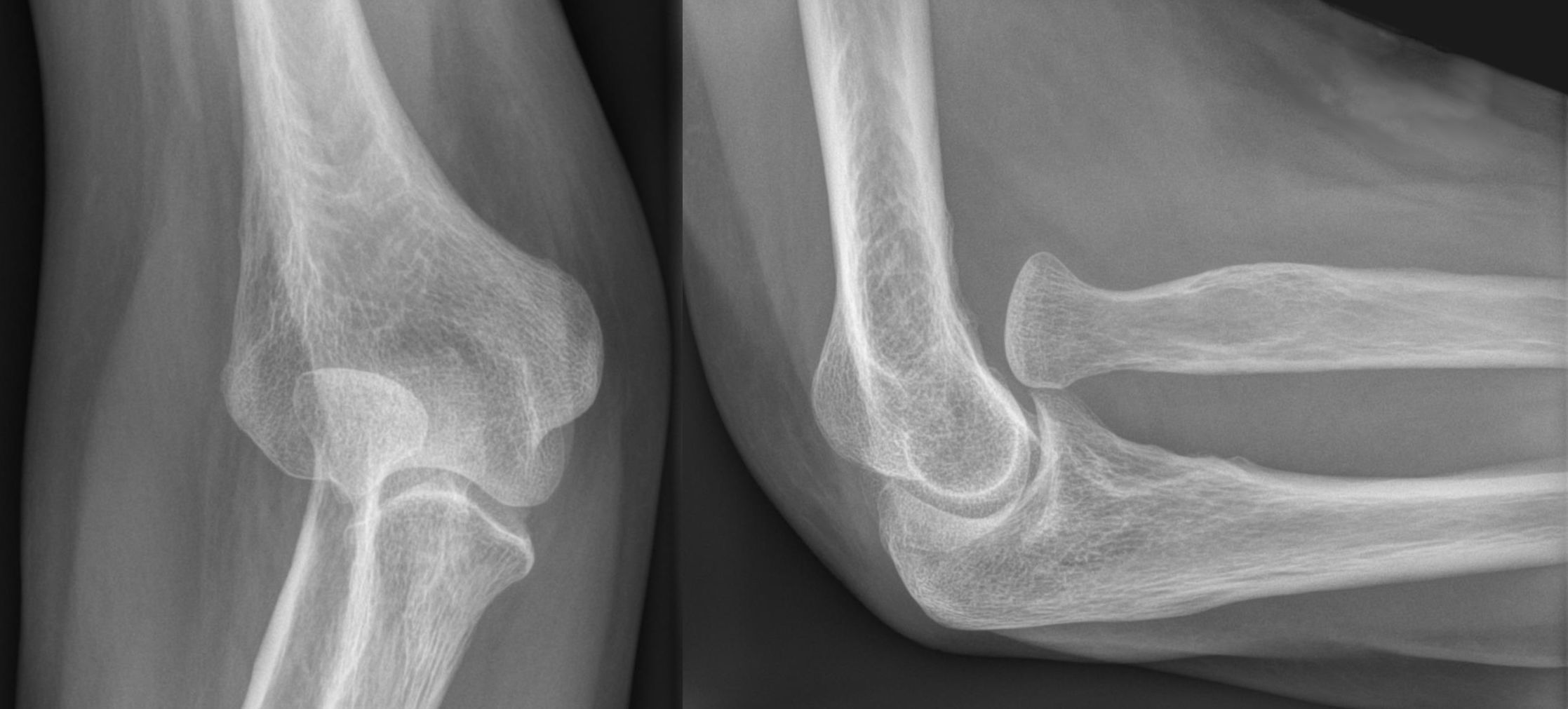
In almost all cases of isolated traumatic radial head dislocation, the radial head is dislocated anteriorly. This is most easily seen in lateral projection, where there is malalignment of the radiocapitellar line - a line drawn down the radial neck should always intersect the capitellum. Where this is lost, radial head dislocation has occurred. If intact, the ulna is likely to be bowed .
In young children it is important to assess the elbow ossification centers to ensure that no other fractures have occurred, e.g. lateral condylar or epicondylar fracture. The mnemonic CRITOE can be used to remember the ossification centers.
In patients with contracture related dislocation (e.g. cerebral palsy), the forearm is pronated by the shortening of pronator teres, and the radial head dislocates posterolaterally .
In brachial plexus palsy related dislocations the direction of dislocation depends on the muscles affected, and can be both anterior or posterolaterally .
Treatment and prognosis
The dislocation needs to be reduced, and sometimes closed reduction is possible. Failing this open reduction will be necessary .
When dislocations of the radial head occur in infancy, the diagnosis may be missed, resulting in chronic radial head dislocation. If this is detected late, it may be potentially confused with congenital radial head dislocation .
In individuals with pronator teres contractures, prophylactic surgical release can be performed to prevent dislocation .
Video tutorial
Siehe auch:
- Monteggia-Fraktur
- Ossifikationszentren Ellenbogen
- kongenitale Radiusköpfchenluxation
- Radius-Capitulum-humeri-Linie
- Radiusköpfchen
- epicondylar fracture
- Radiusköpfchen-Subluxation
- CRITOE
und weiter:


 Assoziationen und Differentialdiagnosen zu Radiusköpfchenluxation:
Assoziationen und Differentialdiagnosen zu Radiusköpfchenluxation:

