renal tuberculosis
Renal tuberculosis, a subset of genitourinary tuberculosis, accounts for 15-20% of extra-pulmonary tuberculosis and can result in varied and striking radiographic appearances.
Tuberculosis can involve both the renal parenchyma and the collecting system (calyces, renal pelvis, ureter, bladder and urethra) and results in different clinical presentations and radiographic appearances. This article focuses on the renal parenchyma, calyces and renal pelvis. For discussion of lower urinary tract and genital involvement please refer to the article on genitourinary tuberculosis.
Clinical presentation
Clinical features are often nonspecific and include:
- hematuria
- flank pain
- constitutional symptoms
Diagnosis can be obtained by culturing multiple first-morning-void urine samples, or by histology of imaging-guided biopsy or surgical specimens, although as with tuberculosis infection elsewhere the diagnosis is not always easy to confirm .
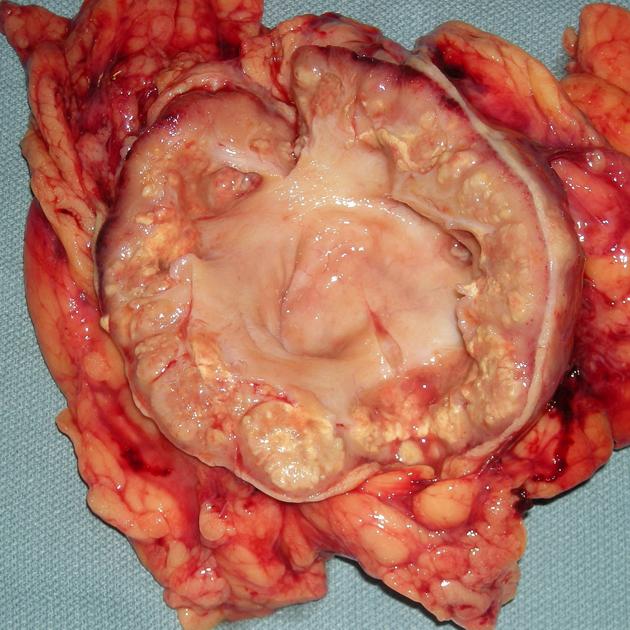
Pathology
Renal infection results from haematogenous spread at the time of primary infection, with multiple micro-abscesses developing at the site of periglomerular capillary seeding. Normal host immunity is usually able to dampen the disease with the usual development of a small inactive granuloma.
Usually there is a long latency between primary infection and presentation which in most case occurs due to host immunity becoming compromised. These quiescent granulomas then can reactivate, grow and eventually communicate with the calyces, leading to downstream infection.
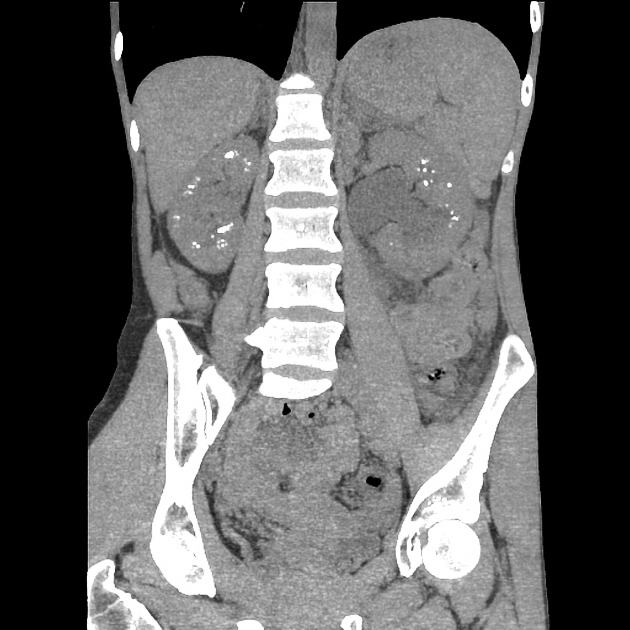
Radiographic features
Both the renal parenchyma and the upper collecting system (calyces and renal pelvis) can be involved. The former is usually seen associated with the latter, which is the most commonly involved site in the genitourinary tract.
Infection limited to the renal parenchyma has two morphological appearances :
- appearances are similar to pyelonephritis caused by other organisms
- hypoperfusion and swelling of all or part of the kidney
- single or multiple nodules
- mimics renal cell carcinoma
Usually the collecting system is involved (either in isolation or in combination with the parenchyma), and appearances vary according to the stage of disease .
- early
- papillary necrosis (single or multiple) resulting in uneven caliectasis
- progressive
- multifocal strictures and hydronephrosis
- mural thickening and enhancement (on cross-sectional imaging)
- end-stage
- progressive hydronephrosis and parenchymal thinning
- dystrophic calcification
- autonephrectomy
Plain radiograph
Plain film findings focus on calcification, which is seen in ~35% (range 25-45%), at various stages of the disease:
- triangular in papillary necrosis
- focal or amorphous: putty kidney (end-stage)
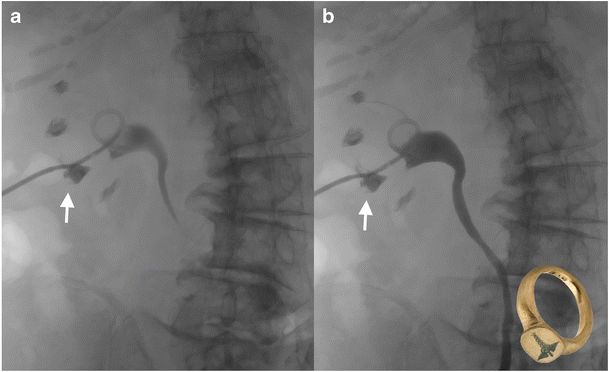
Fluoroscopy
Traditional plain film IVP is quite sensitive to renal tuberculosis with only 10% of affected patients having normal imaging. Features include:
- parenchymal scars 50%
- moth eaten calyces: early finding
- irregular caliectasis
- phantom calyx
- hydronephrosis
Lower urinary tract signs (see bladder and ureteral tuberculosis) also recognized include:
- Kerr kink
- sawtooth ureter
- pipe-stem ureter
- beaded or corkscrew ureter
- thimble bladder
Ultrasound
Sonographic appearances are nonspecific and variable, depending on the stage of the disease.
- early
- normal kidney or small focal cortical lesions with poorly defined border
- +/- calcification
- progressive
- papillary destruction with echogenic masses near calyces
- distorted renal parenchyma
- irregular hypoechoic masses connecting to collecting system; no renal pelvic dilatation
- mucosal thickening +/- ureteric and bladder involvement
- small, fibrotic thick-walled bladder
- echogenic foci or calcification (granulomas) in bladder wall near ureteric orifice
- localized or generalized pyonephrosis
- end-stage
- small, shrunken kidney, "paper-thin" cortex and dense dystrophic calcification in collecting system
- may resemble chronic renal disease
Ultrasound is less sensitive than CT in detection of:
- calyceal, pelvic or ureteral abnormalities
- isoechoic parenchymal masses
- small calcifications
- small cavities that communicate with collecting system
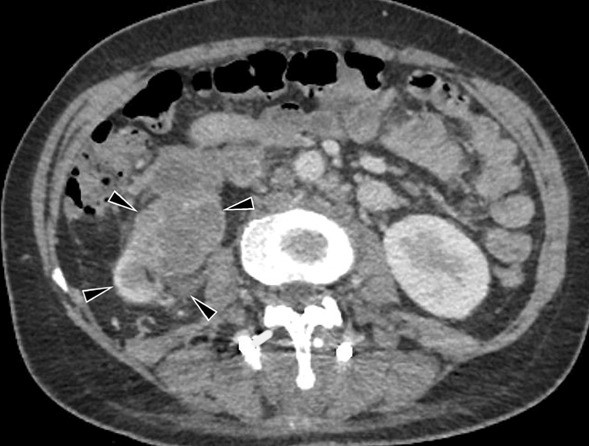
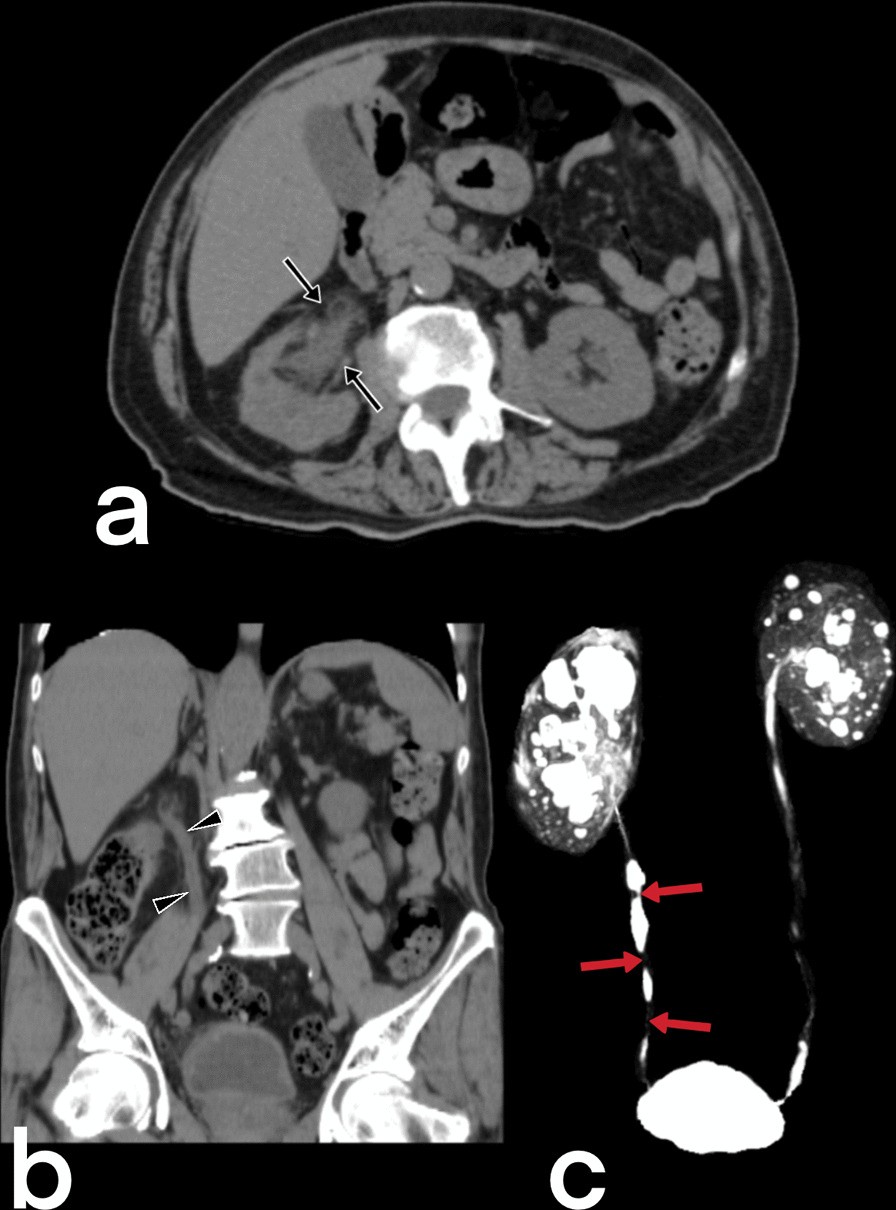
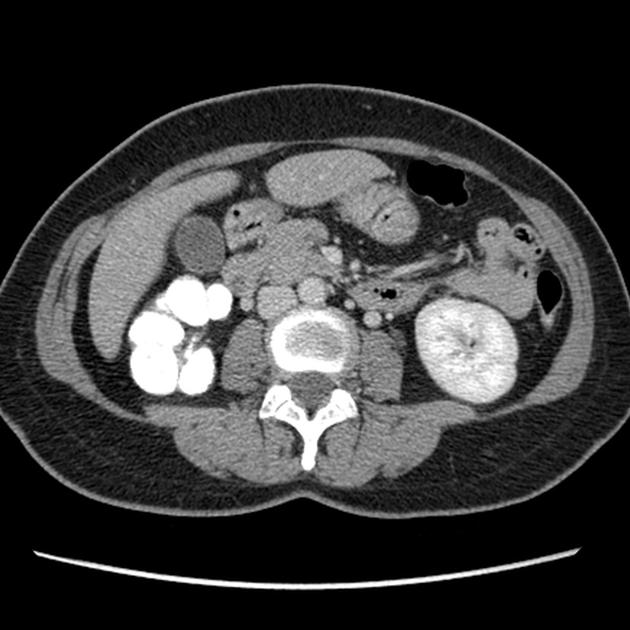
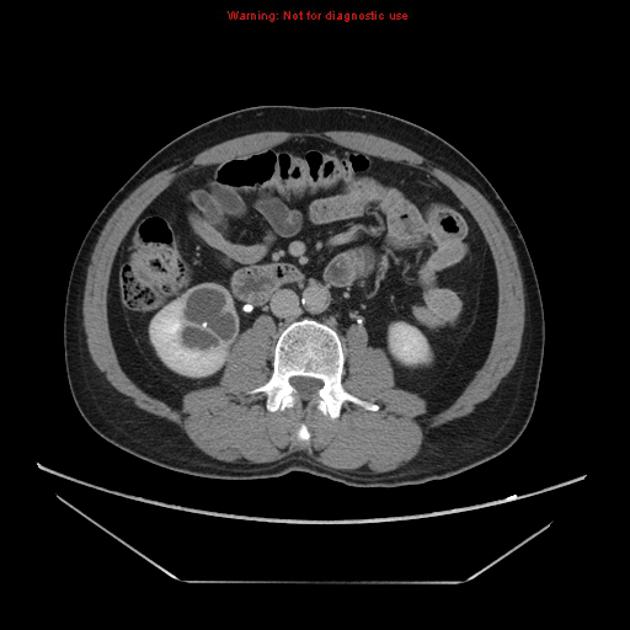
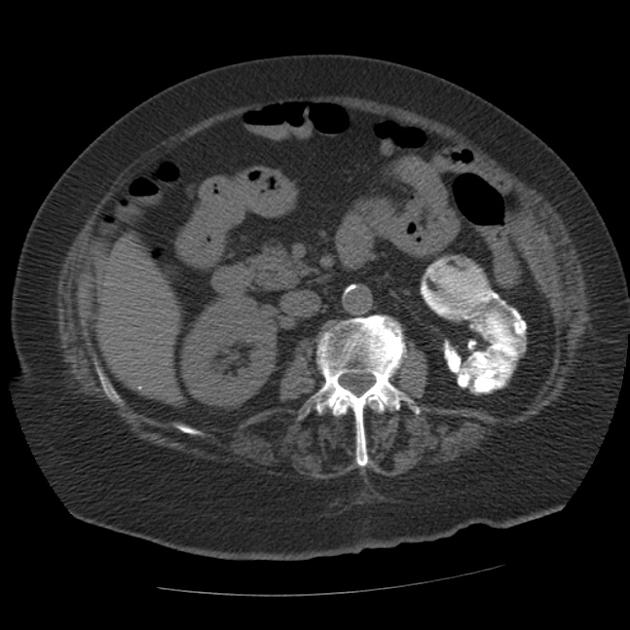
CT
CT is the most sensitive modality for visualizing renal calcifications and CT IVP is more sensitive at identifying all manifestations of renal tuberculosis .
- early
- papillary necrosis (single or multiple) resulting in uneven caliectasis
- progressive
- multifocal strictures can affect any part of the collecting system
- generalized or focal hydronephrosis
- mural thickening and enhancement
- poorly enhancing renal parenchyma, either due to direct involvement or due to hydronephrosis
- end-stage
- progressive hydronephrosis results in very thin parenchyma, mimicking multiple thin-walled cysts
- amorphous dystrophic calcification eventually involves the entire kidney (known as putty kidney)
Treatment and prognosis
Multi-drug treatment is essential, however despite treatment, stricturing can progress.
The role of nephrectomy is controversial and depends on the degree of renal impairment, bilateral vs unilateral disease and the status of the lower urinary tract. Nephrectomy, partial nephrectomy or cavernostomy can be performed both open and endoscopically .
Differential diagnosis
General imaging differential considerations include:
- papillary necrosis
- medullary sponge kidney
- TCC (transitional cell carcinoma) of renal tract
- SCC (squamous cell carcinoma) of renal tract
- xanthogranulomatous pyelonephritis (XGP)
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Nierentuberkulose:
Assoziationen und Differentialdiagnosen zu Nierentuberkulose: