Resorptive (obstructive) atelectasis
Resorptive or obstructive atelectasis is a form of lung collapse that is due to obstruction of the airways supplying a lung segment or lobe. It is a term used to distinguish atelectasis identified on imaging based on the underlying pathophysiology to guide diagnosis.
Clinical presentation
The presentation of patients with atelectasis depends on the underlying cause. However, breathlessness is common if there is significant lung collapse and infective symptoms can be present if there is co-existing sepsis.
Pathology
As the name implies, in this form of atelectasis there is partial or complete bronchial obstruction which leads to poor ventilation of the airways supplied. As ventilation between the distal air spaces and the trachea is disrupted the residual air in the affected lung is resorbed by the circulating blood at a rate greater than it is replaced by fresh ventilated air. This causes volume loss in the affected lung. Volume loss may be minimal in distal airways obstruction due to the presence of collateral ventilation via the pores of Kohn.
The rate at which atelectasis progresses depends on whether there is obstruction of a lobar or segmental bronchus. Lobar obstruction manifests as lobar atelectasis. In segmental atelectasis, there is often a degree of collateral ventilation from adjacent lung segments which causes a slightly distinct radiographic presentation. The speed of collapse is quicker if the patient is being given 100% oxygen .
Collapse occurs quickly if the obstruction is due to a luminal lesion that can act as a one-way valve.
Eventually, there can be sequestration of local lung secretions over time and areas of significant atelectasis are prone to become infected. Hence, this type of collapse is frequently seen with co-existing consolidation.
Etiology
The causes of resorption (obstructive) atelectasis can be thought of in terms of where the obstructing lesion arising from with respect to the bronchial lumen:
- extra-luminal
- neoplasm
- lymphadenopathy
- bronchial
- fibrotic stricture
- neoplasm
- spontaneous rupture
- luminal
- mucus plugging
- pus
- bacterial pneumonia
- blood
- post-traumatic lung injury
- foreign body
- endobronchial intubation
Radiographic features
Plain radiograph / CT
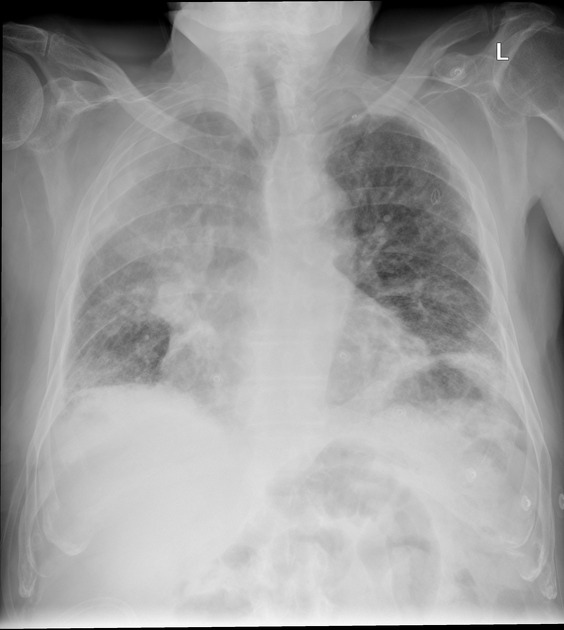
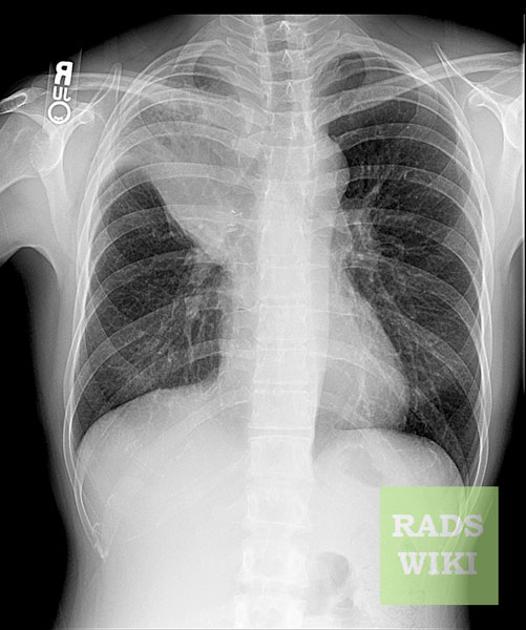
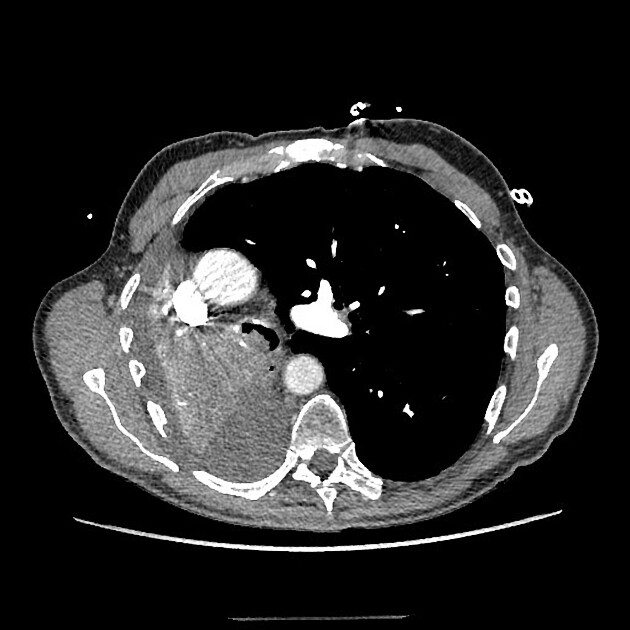
The imaging features of atelectasis are similar on plain radiographs and CT with more detail being available on the CT:
- increased density at the site of atelectasis
- loss of normal thoracic silhouettes
- displacement of the fissures toward the area of atelectasis
- upward displacement of ipsilateral hemidiaphragm
- crowding of pulmonary vessels and bronchi affected area
- compensatory hyperinflation of the unaffected lung
- mediastinal shift
- ipsilateral tracheal deviation
- ipsilateral shift of the heart
If volume loss is minimal and there is consolidation present, then the term drowned lung can be used to indicate transudate replacing the air in the collapsing lung. The transudate is rapidly cleared when the obstruction is removed, as is commonly seen in postoperative patients with mucous plugging.
Ultrasound
As a consequence of the cessation of ventilation, lung sliding is immediately abolished. In contrast to a pneumothorax, another cause of absent lung sliding, the presence of a lung pulse implies that the visceral and parietal pleura are still in apposition. As alveolar gas is absorbed, the lung parenchyma may assume a tissue-like echogenicity, with the following internal features ;
- air bronchograms
- unlike dynamic air bronchograms (present in e.g. pneumonia) these lentiform, branching echogenicities do not move with respiration
- referred to as static air bronchograms
- fluid bronchograms
- tubular hypoechoic structures lacking vascular flow on color Doppler

