skeletal sarcoidosis



Skeletal sarcoidosis is an uncommon manifestation of sarcoidosis.
Epidemiology
Skeletal involvement is thought to occur in ~1-13% of patients with sarcoidosis .
Osseous involvement may be more common in black patients .
Clinical presentation
Patients with large bone lesions and vertebral lesions may become symptomatic. The exact symptoms may vary depending on site. It may be accompanied by lupus pernio (chronic, predominantly facial skin lesion resembling frostbite ) or other types of infiltrative skin lesions .
Pathology
Primary skeletal involvement without other organ involvement is extremely rare . Approximately 80-90% patients have concurrent pulmonary involvement .
Location
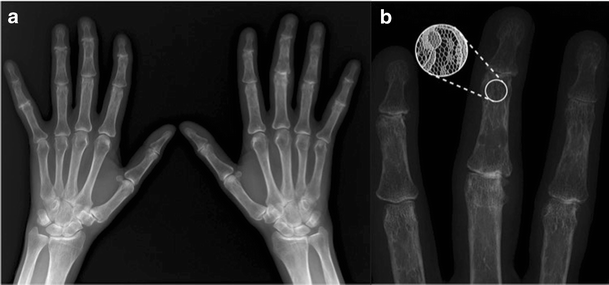
The phalanges in the hands and feet are most frequently affected. There is typically multiple joint involvement.
Radiographic features
Plain radiograph
Small bone lesions
Radiographic features may include cyst-like radiolucent areas, a lacelike honeycomb appearance (this is typically seen in the hands), or extensive bone erosion with pathologic fractures. The articular spaces are usually intact unless extensive neuropathic lesions develop. A subcutaneous soft-tissue mass or tenosynovitis may also be present.
When there is involvement of other skeletal structures, diagnosis becomes difficult as the condition can mimic various other pathology
Large bone lesions and axial skeletal lesions
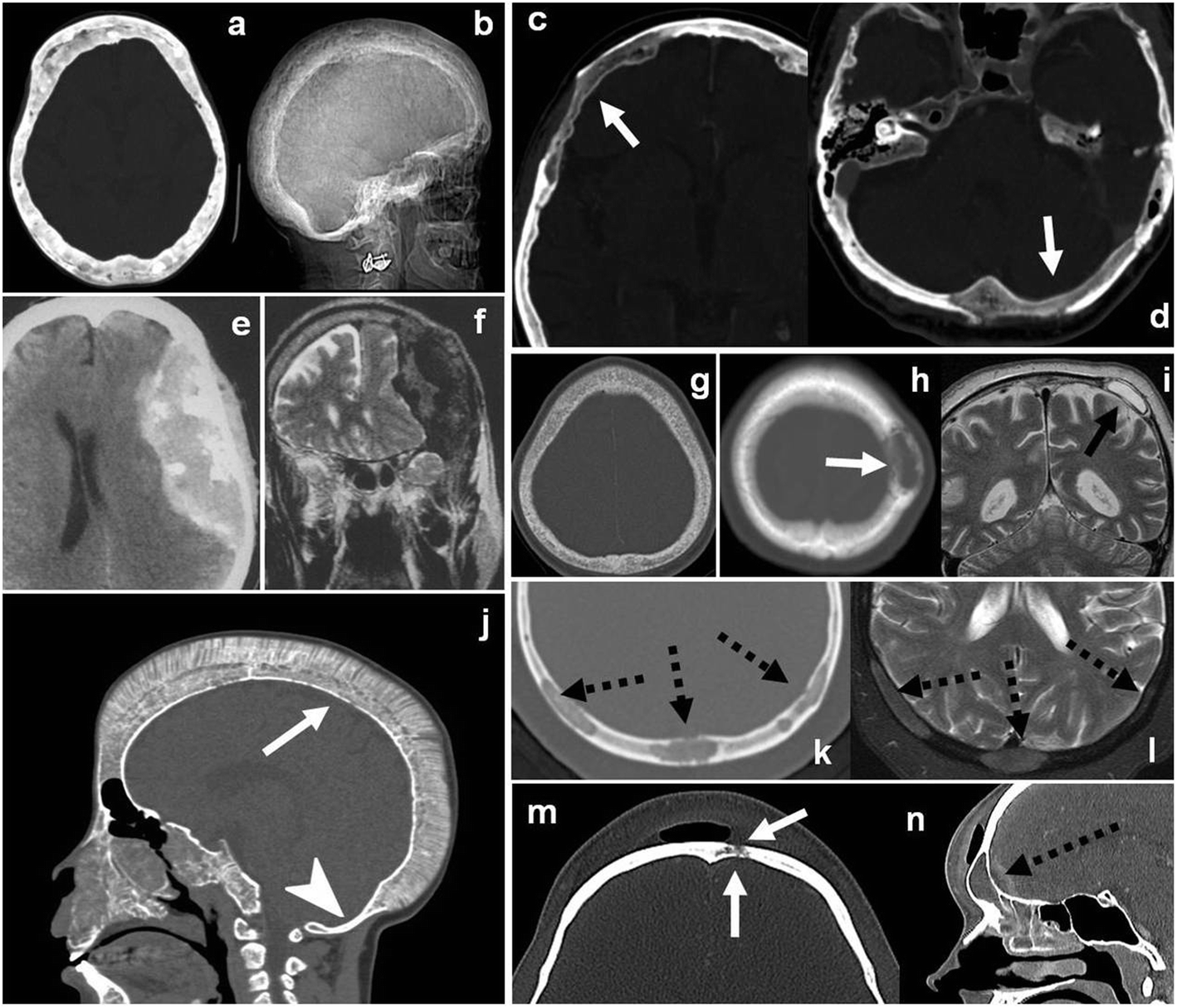
Large bone lesions may manifest radiographically as either focal lytic or sclerotic areas. They may even be occult.
In the vertebrae, sarcoidosis can cause osteolytic lesions and disc spaces are usually preserved. Widespread vertebral sclerosis can also occur.
They have been secondary alignment abnormalities deformities due to pathologic fractures with bone collapse.
MRI
MRI may demonstrate fine perpendicular lines extending from the ghost of the cortex and resembling periostitis .
Intermediate-density–weighted MR imaging sarcoidal nodules are typically hyperintense .
MR imaging of large bony lesions usually reveals indistinct or well-marginated lesions of varying sizes.
Reported signal characteristics include:
- T1: large bone lesions are typical low signal
- inversion recovery: can have high signal
- T2 / PD FS: most cases are high signal
- C+ (Gd): lesions may enhance
Nuclear medicine
Scintigraphic findings become usually positive even before the lesions become manifest at radiography. Both Tcm methylene diphosphonate and Ga citrate imaging may show uptake.
PET/CT
FDG-PET/CT has shown promising results in the detection of extra-thoracic involvement including skeletal lesions .
Differential diagnosis
While classical hand lesions have characteristic features, there is a wide differential for skeletal involvement in other sites
For vertebral lesions, consider
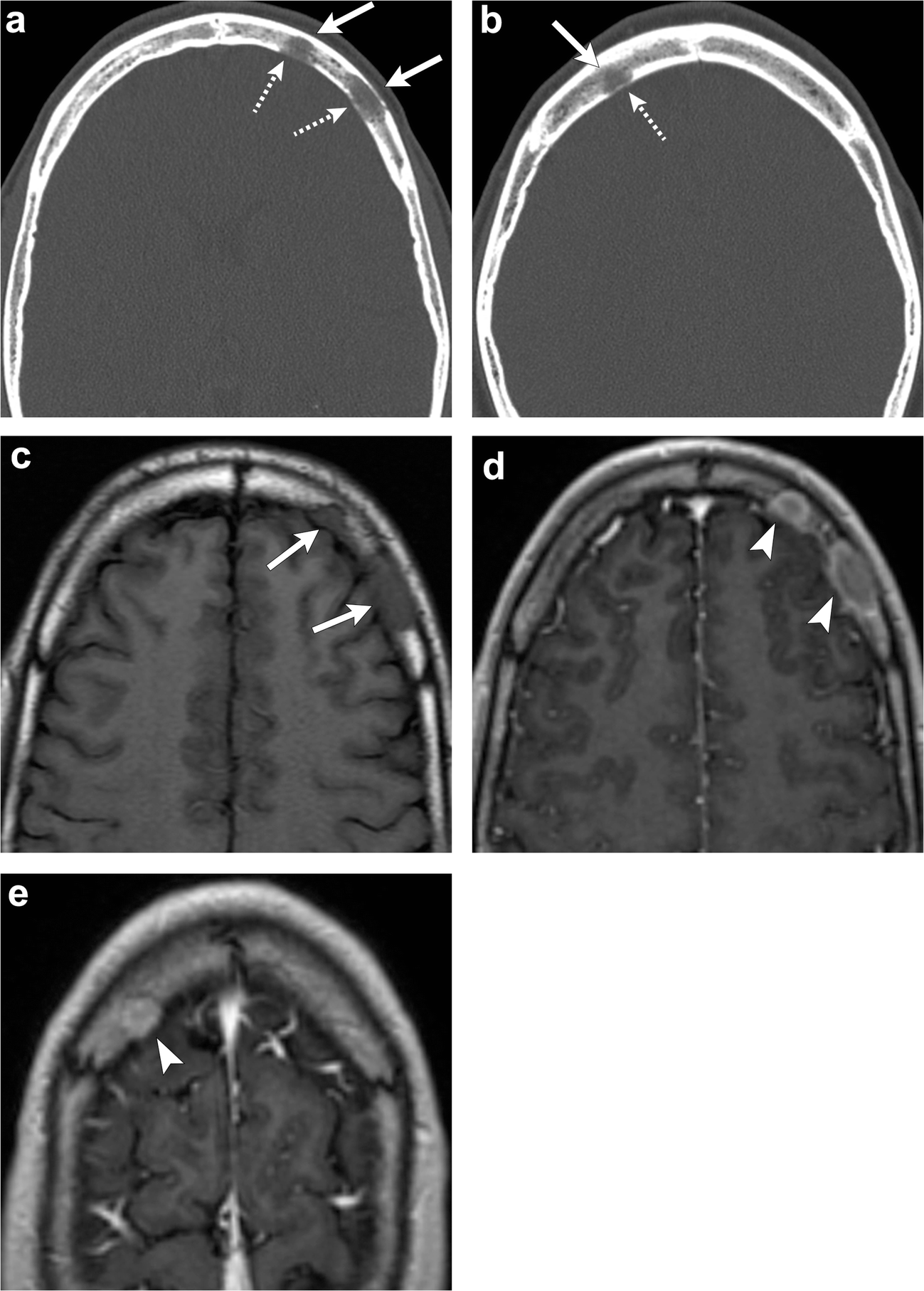
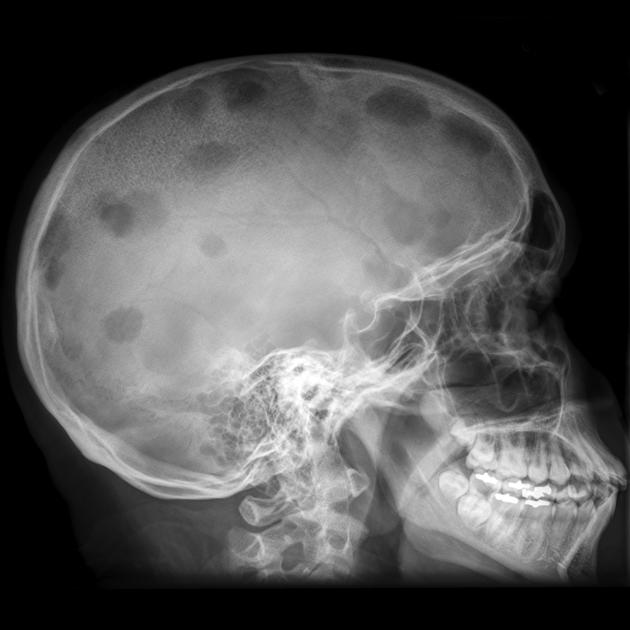
For calvarial lesions also additionally consider
See also
Siehe auch:
- Sarkoidose
- vertebrale Metastasen
- Multiples Myelom
- benigne Osteolysen
- musculoskeletal manifestations of sarcoidosis
- skeletale Manifestationen der Langerhanszell-Histiozytose
- Sarkoidose der Kalotte
und weiter:


 Assoziationen und Differentialdiagnosen zu Sarkoidose ossäre Manifestationen:
Assoziationen und Differentialdiagnosen zu Sarkoidose ossäre Manifestationen:



