cardiac bronchus
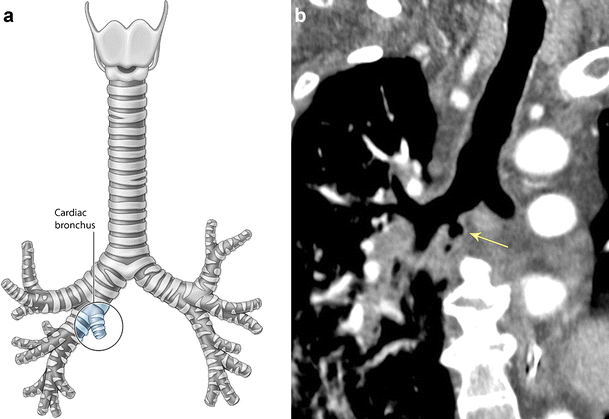
A cardiac bronchus (or sometimes termed accessory cardiac bronchus (ACB)) is a rare anatomic variant of the tracheobronchial tree, arising from the medial aspect of the bronchus intermedius.
Epidemiology
This anomaly is rare and is reported in ~0.3% (range 0.09-0.5%) of individuals . There may be a predilection for males.
Clinical presentation
The vast majority of cardiac bronchi are asymptomatic. In some patients with lung parenchyma supplied by this bronchus, abnormal drainage predisposes to repeated chest infection . Hemoptysis as well as cases of malignant transformation have also been described.
Pathology
The anomaly is thought to occur between the 4 and 6 weeks of gestation, during development of the bronchial tree .
The histology of its wall is that of normal airway.
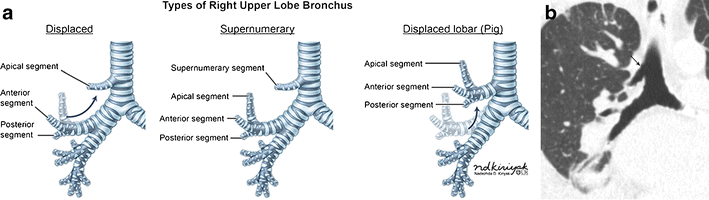
A cardiac bronchus arises from the bronchus intermedius, opposite and just distal to the origin of the right upper lobe bronchus. It is variable in size, morphology and length (range from 0.5-5 cm) . In about half of cases, the cardiac bronchus is a short blind-ending bronchial stump with no branches and does not supply any lung parenchyma. In the remainder, the bronchus may have branches and an amount of aerated lung parenchyma .
It is the only recognized true supernumerary bronchus, with other anomalies representing aplasia or abnormal branching patterns .
Radiographic features
CT
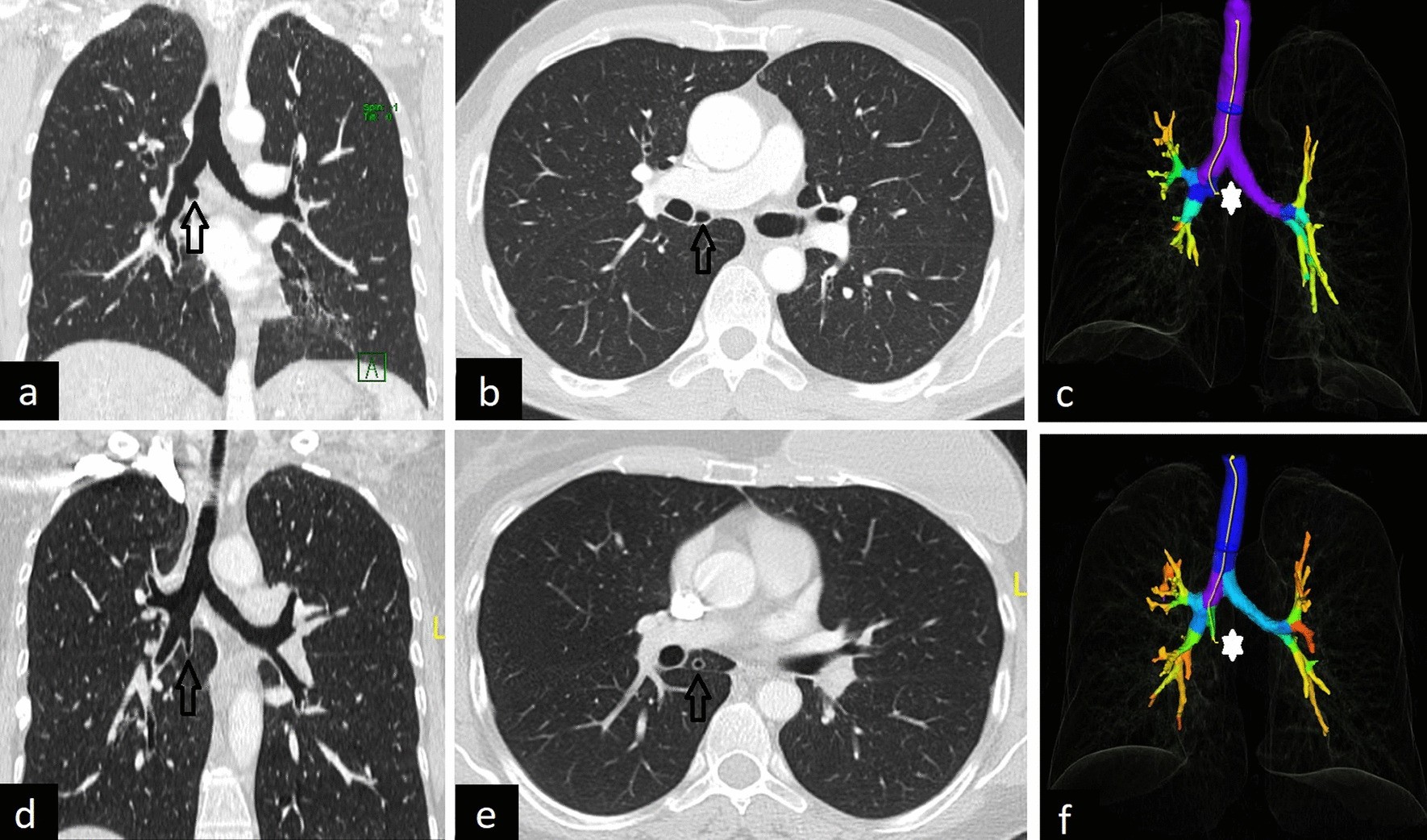
A cardiac bronchus is almost always an incidental finding of CT examination of the chest. It appears as a continuation of the lumen of the bronchus intermedius, projecting medially and directly inferiorly towards the posterior aspect of the heart in a caudal direction.
In some cases, the dependent lung parenchyma may be collapsed and mimic a soft tissue mass .
Treatment and prognosis
As these structures are usually asymptomatic, no treatment is required. In rare instances where recurrent infections can be attributed to a cardiac bronchus then surgical resection may be carried out .
History and etymology
It is thought to be first described by RC Brock in 1946 .
Differential diagnosis
There is usually little, if any, differential diagnosis as most cases are classical in appearance. In atypical cases, differential includes:
- tracheobronchial diverticulum
- different histologically: diverticula do not have normal bronchial wall morphology
- bronchial laceration in trauma
- almost always associated with other chest traumatic injuries
- necrotic/cavitating mass
- a consideration when associated lung parenchyma is atelectatic
Practical points
- owing to the possible complications mentioned above, the role of the radiologist is to both identify and report this rare anomaly
- bronchoscopy may be indicated to differentiate the entity from a diverticulum
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Bronchus cardiacus:
Assoziationen und Differentialdiagnosen zu Bronchus cardiacus: