cholesteatoma



Cholesteatomas are histologically-equivalent to an epidermoid cyst and are composed of desquamated keratinizing stratified squamous epithelium forming a mass.
Clinical presentation
They may be asymptomatic, or may present with conductive hearing loss, dizziness, or otorrhea.
Pathology
The mass is lined by epithelium (facing inwards) which continues to grow, thereby shedding additional cells into the mass. Their cholesterol content (which is not always present) is responsible for their name, although 'keratoma' is probably a more apt term.
Cholesteatomas of the temporal bone and middle ear can be divided into:
- congenital cholesteatoma: accounting for only 2%
- acquired cholesteatoma: 98%
- primary (no history of chronic otomastoiditis)
- secondary (the vast majority):
- external ear canal cholesteatoma
- mural cholesteatoma
- petrous apex cholesteatoma
Radiographic features
MRI
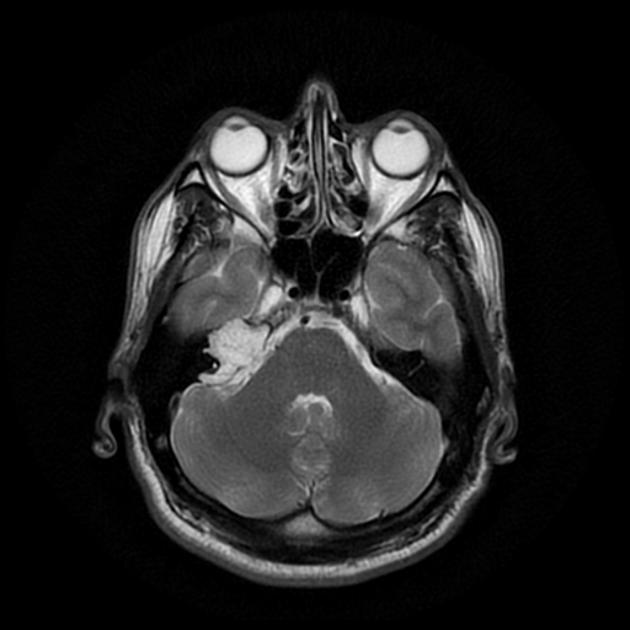
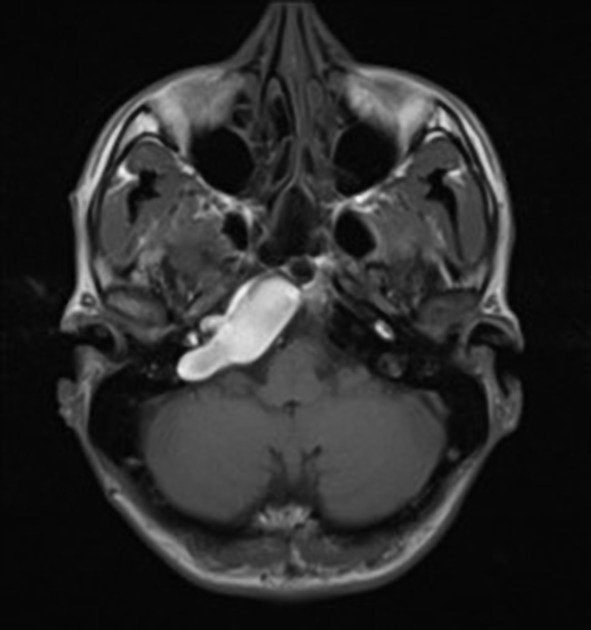
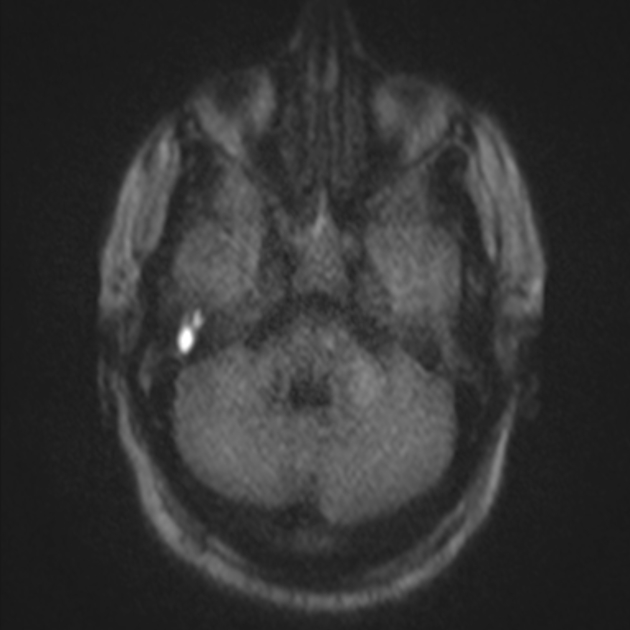
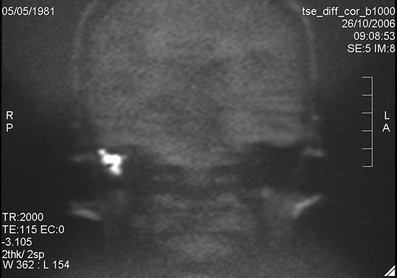
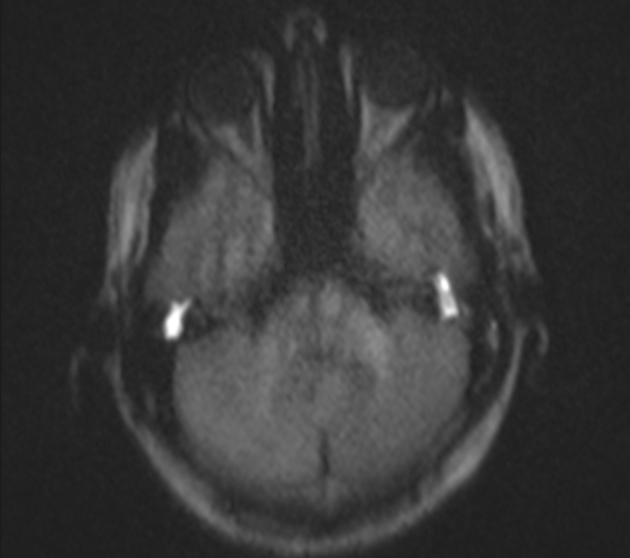
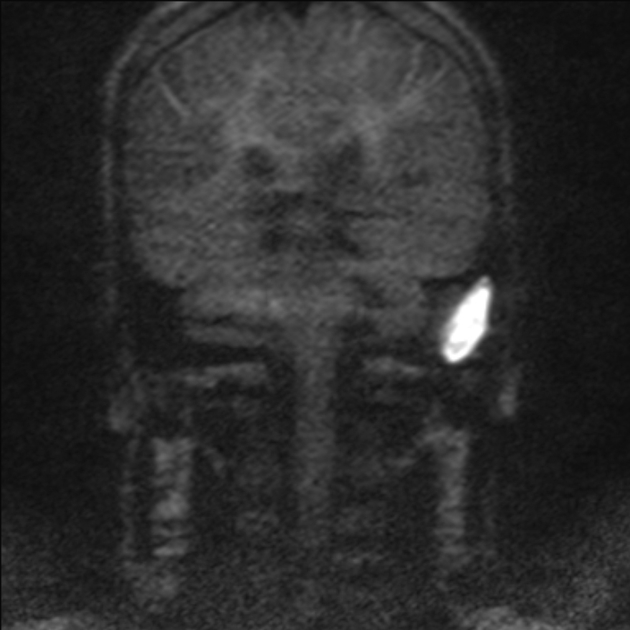
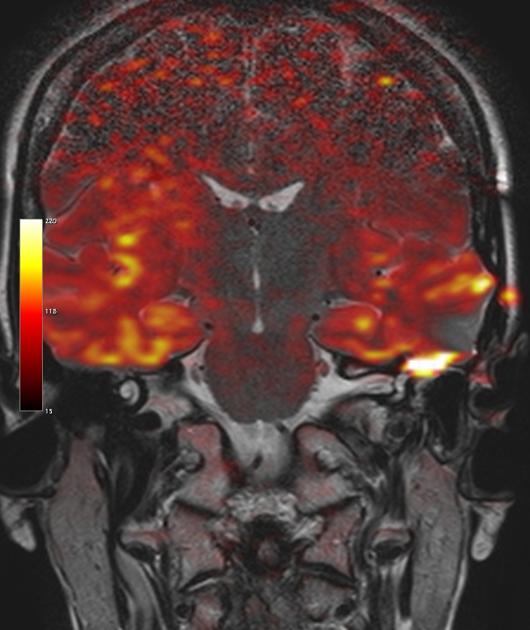
Conventional non-contrast MR imaging with diffusion-weighted imaging is recommended in all patients with a suspicion of cholesteatoma. An MRI should be performed especially in patients with previous surgery for cholesteatoma since recurrence or residual tumor can be detected with great accuracy. If negative, it can obviate "second look" surgery. It is important to prepare the patient for the examination (clear the external auditory canal or the postoperative cavity) to avoid a false positive diagnosis.
The standard examination is a T2-weighted series in the coronal and axial plane, followed by a non-echo planar DWI series (b-values 0, 1000). On the DWI images with b-value 1000 s/mm, a cholesteatoma becomes apparent as a hyperintense area. The signal intensity should be higher than visible on the DWI images with b-value 0 s/mm. On the ADC map, a low signal should be visible in the same area, confirming the presence of diffusion restriction.
With these findings, recurrent cholesteatoma can be detected with 100% specificity. Cholesteatomas down to a size of 2 mm can be detected with this technique on a 1.5 T MRI machine.
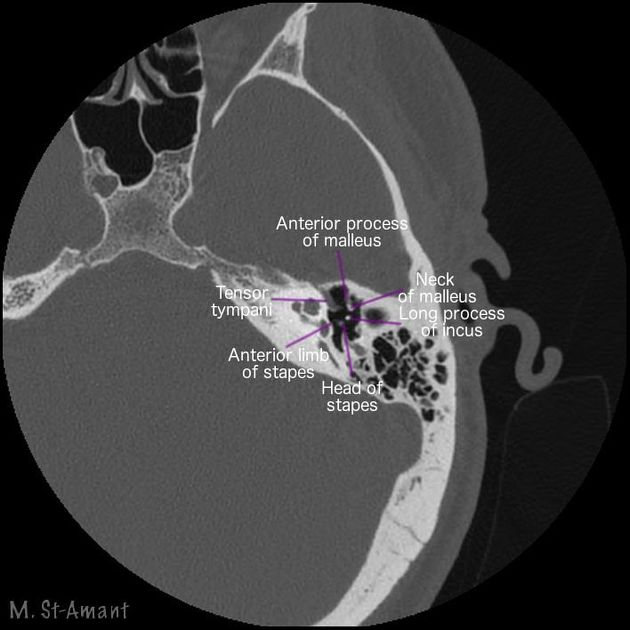
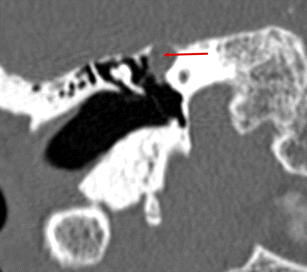
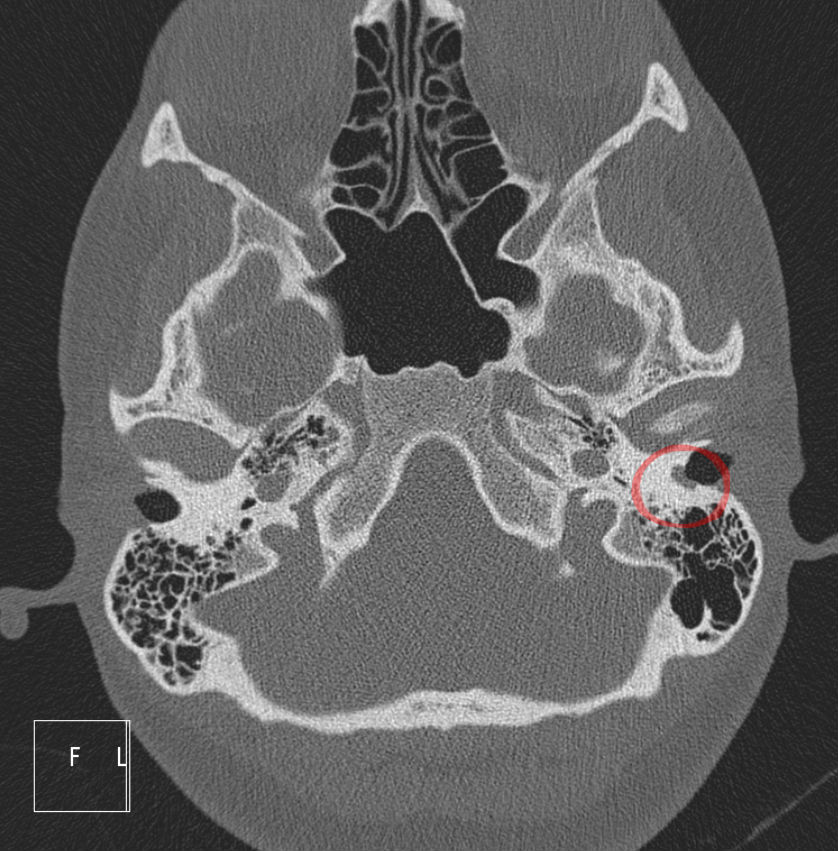
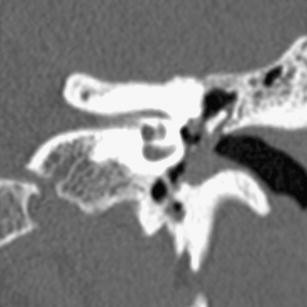
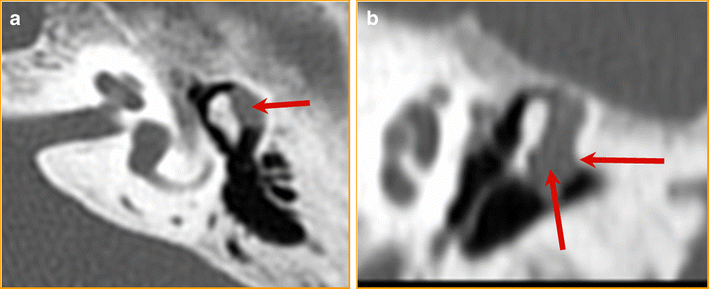
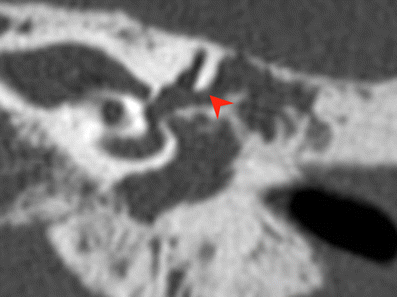
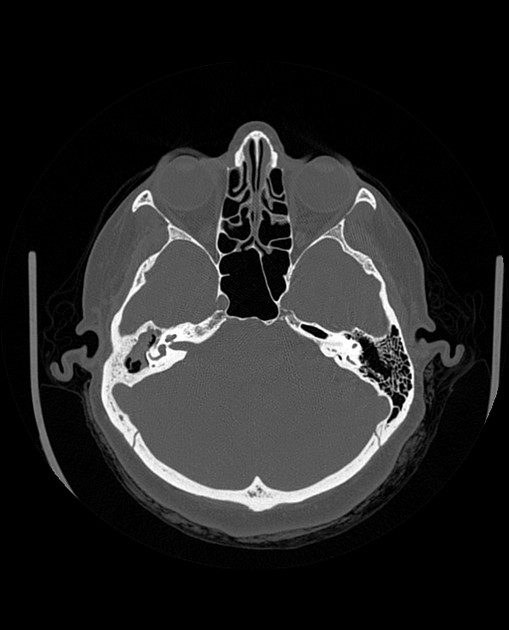
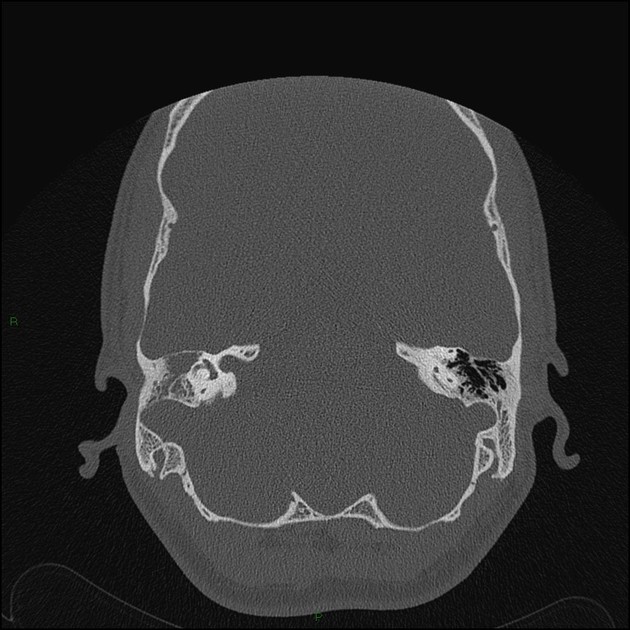
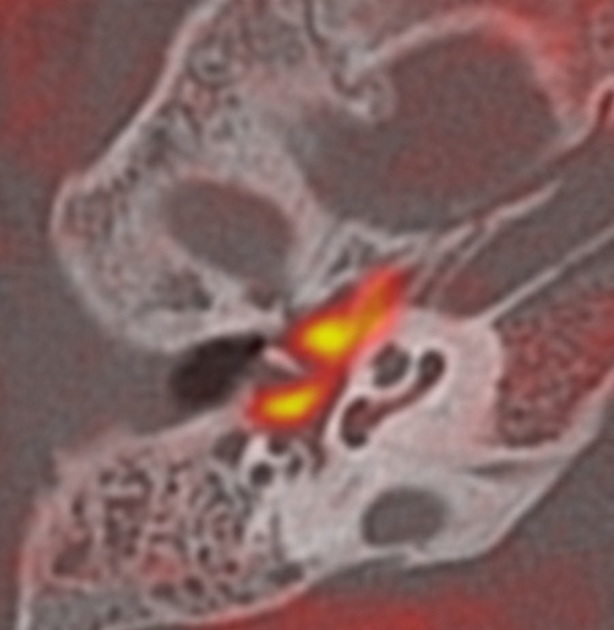
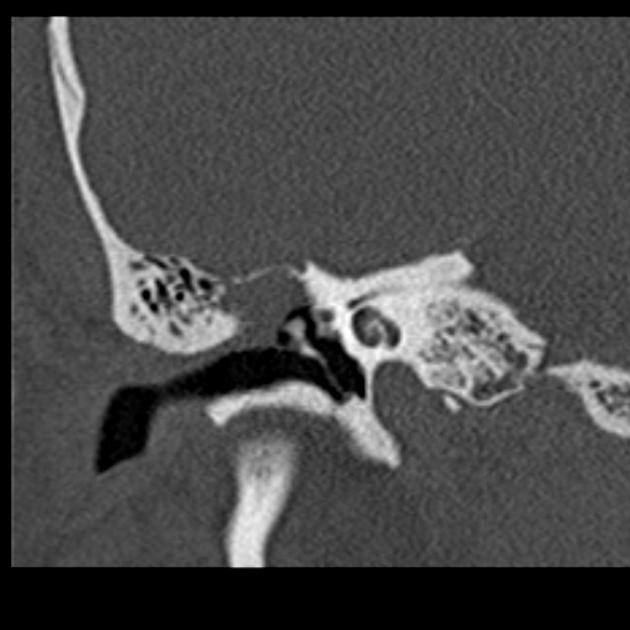
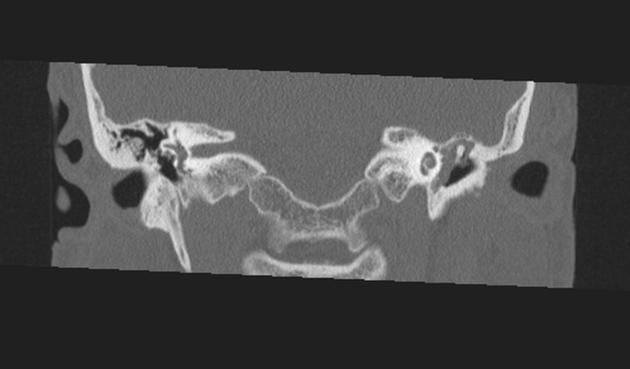
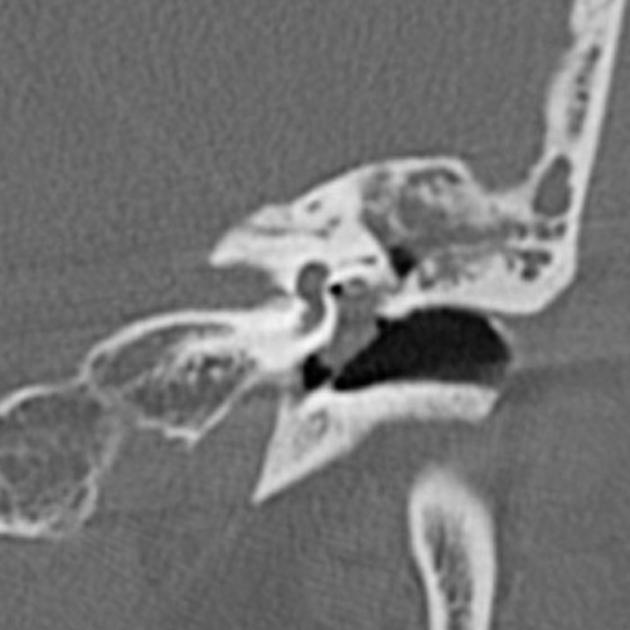
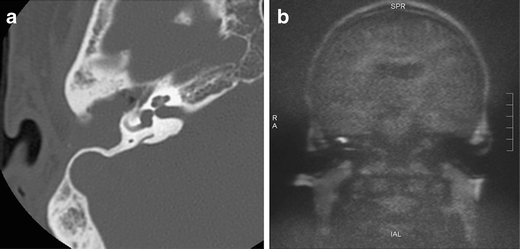
CT
A CT scan should be added in those cases where a cholesteatoma is detected with MRI. CT is required for preoperative planning (reconstruction of ossicles if needed) and to exclude perforation of the bony tegmen.
The pars flaccida cholesteatoma originates in Prussak space and usually extends posteriorly, while the pars tensa cholesteatoma originates in the posterior mesotympanum and tends to extend posteromedially.
Treatment and prognosis
Generally, surgical excision is eventually necessary . Excision is often performed with tympanoplasty ± mastoidectomy ± ossicular reconstruction, depending on extent of disease .
Differential diagnosis
The main differentials, which unlike cholesteatoma show a high signal on the ADC map, are:
- cholesterol granuloma
- inflammation
Further differential diagnoses include:
- cerumen: which shows similar image characteristics to cholesteatoma but is located in the external ear canal
- abscess formation in the middle ear: can also show similar imaging findings but has a completely different clinical presentation
Practical points
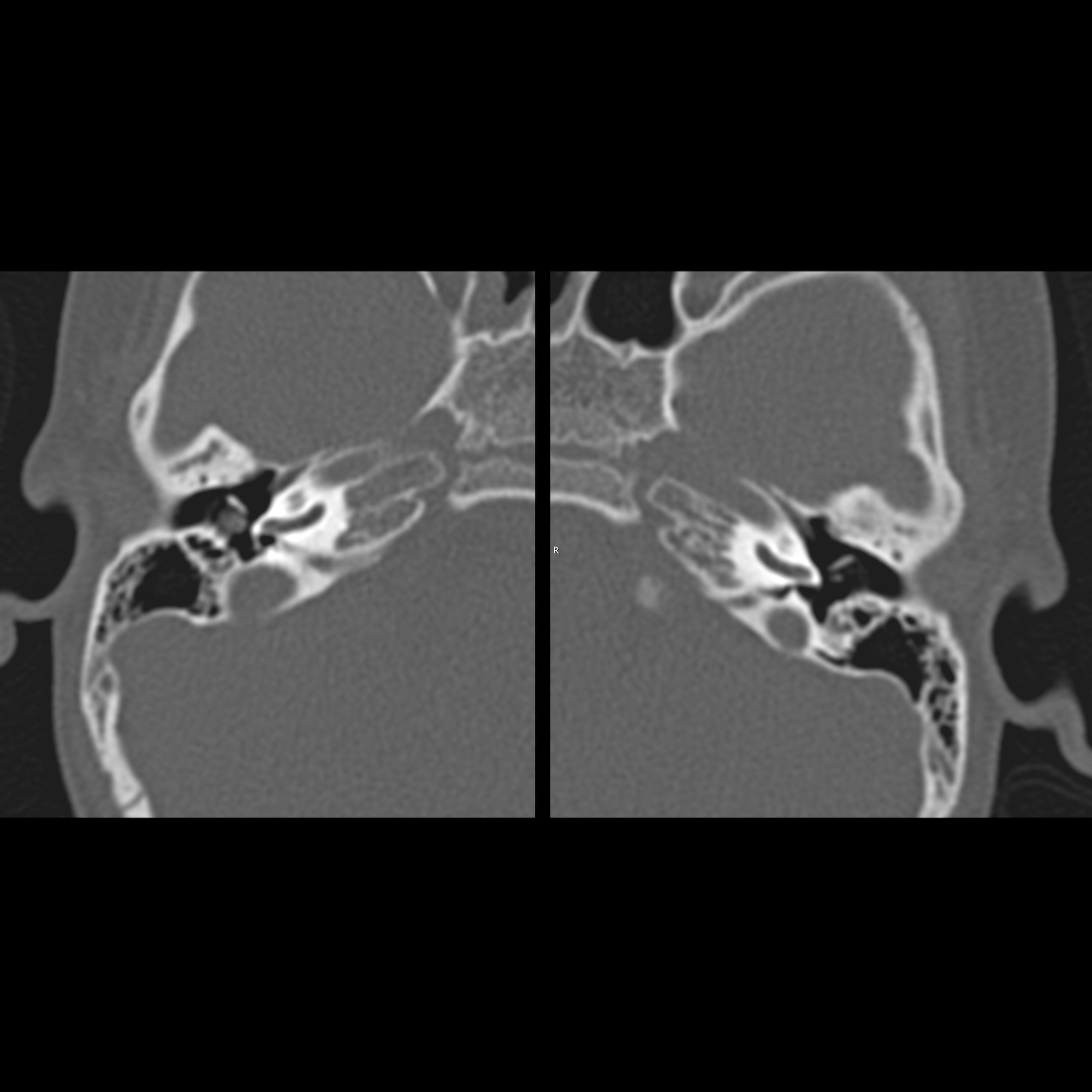
Important CT features to comment on when reporting a cholesteatoma:
- erosions of the
- dehiscence of the
- the integrity of the
- epitympanum
- aditus ad antrum and mastoid antrum
- oval and round window
- the presence of cholesteatoma in the sinus tympani (which is the most hidden recess of the middle ear): to avoid residual disease
Siehe auch:
- Cavum tympani
- Cholesterolgranulom der Felsenbeinspitze
- chronische Otomastoiditis
- Chordom
- Chondroblastom
- Schwannom
- Riesenzelltumor
- Otitis media
- Paragangliom
- Metastase
- Histiozytose X
- Cholesteatom des äußeren Gehörgangs
- erworbenes Cholesteatom
- congenital cholesteatoma
- epidermale Inklusionszyste
- Primitiver neuroektodermaler Tumor
- Schwannom des Nervus facialis
und weiter:
- Labyrinthitis
- Spasmus hemifacialis
- middle ear cholesteatomas
- chronische Mittelohrentzündung
- fistula test
- Raumforderung Felsenbein
- acquired middle ear cholesteatoma
- Flüssigkeit in den Mastodzellen
- recurrent cholesteatoma
- Cholesteatom mit Infiltration Nervus facialis
- pars tensa cholesteatoma
- Frakturen Os temporale


 Assoziationen und Differentialdiagnosen zu middle ear cholesteatomas:
Assoziationen und Differentialdiagnosen zu middle ear cholesteatomas: