choroid plexus carcinoma



Choroid plexus carcinomas are malignant neoplasms arising from the choroid plexus. They are classified as a WHO grade III tumor and while there is considerable overlap in imaging characteristics it carries significantly poorer prognosis than both WHO grade II atypical choroid plexus papilloma, and WHO grade I choroid plexus papilloma.
Epidemiology
Choroid plexus carcinomas occur predominantly in children, typically in the first 5 years of life. They are rare, far less common than choroid plexus papillomas (which account for 80% of primary choroid plexus tumors), representing only 1-4% of pediatric brain tumors .
Clinical presentation
As is the case with choroid plexus papillomas, presentation usually is as a result of hydrocephalus. Symptoms include increasing head circumference and headaches. Papilledema may be visible on fundoscopy. In addition, choroid plexus carcinomas have a tendency to invade the adjacent brain and thus may present with focal neurological dysfunction .
Associations
- Li-Fraumeni syndrome
- Aicardi syndrome
- simian virus 40 (SV40) on the basis of this virus' DNA having been identified in up to 50% of cases
Pathology
They originate from choroid plexus epithelium and typically arise de novo; rarely they may represent malignant transformation of a pre-existing choroid plexus papilloma .
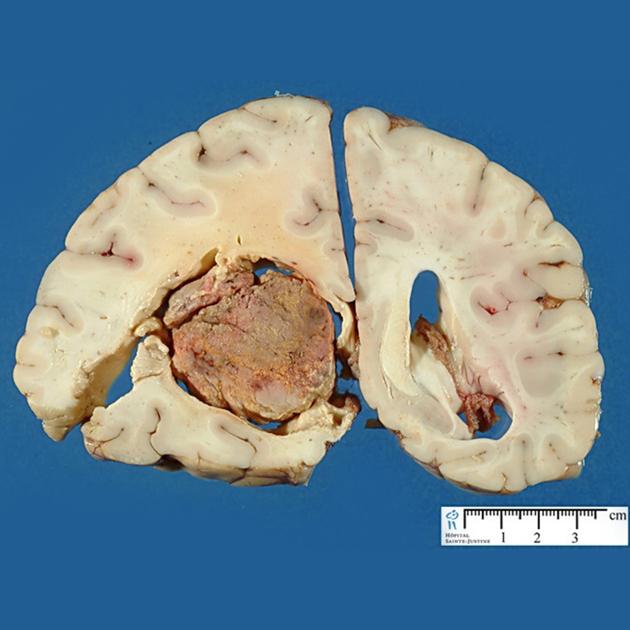
Macroscopic appearance
Macroscopically, choroid plexus carcinomas are lobulated masses with cystic and necrotic areas.
Microscopic appearance
It has been suggested that to make the diagnosis of choroid plexus carcinoma, at least 4 of the following 5 features should be present :
- increased mitotic rate: >5 per 10 high-power fields
- increased cellularity
- nuclear pleomorphism
- necrosis
- blurred papillary structure
Microcalcifications and hemorrhage may be present. Brain parenchymal invasion is a feature, and if present helps to distinguishes choroid plexus carcinomas from choroid plexus papillomas.
Immunophenotype
The immunophenotype of choroid plexus carcinomas is similar to that of choroid plexus papillomas, with both S11 and transthyretin more likely to be negative .
- cytokeratins: positive
- S100: often negative
- transthyretin: often negative
- EMA: negative
- p53 protein: positive in individuals with TP53 mutation
- KIR7.1: only positive in ~50% of cases
Genetic markers
The most common underlying genetic mechanism identified in their formation is dysfunction of the p53 tumor suppressor gene (TP53).
Radiographic features
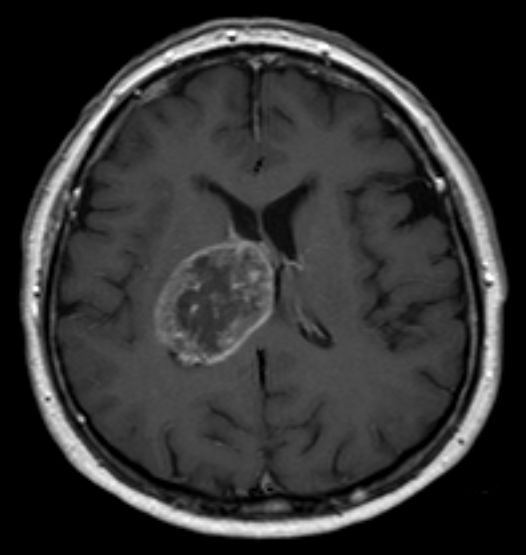
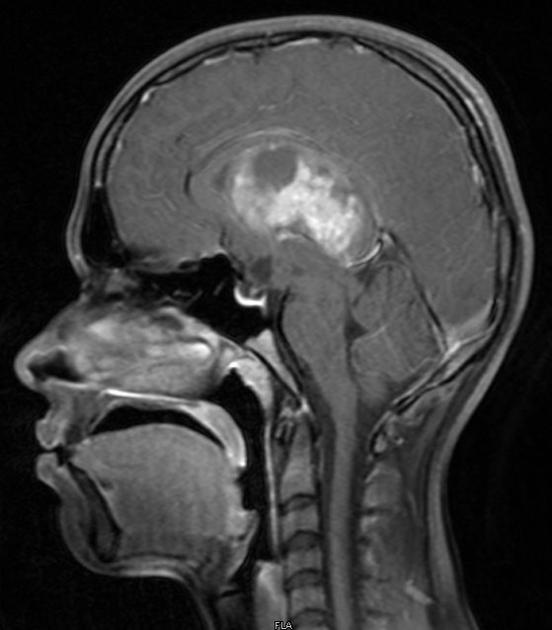
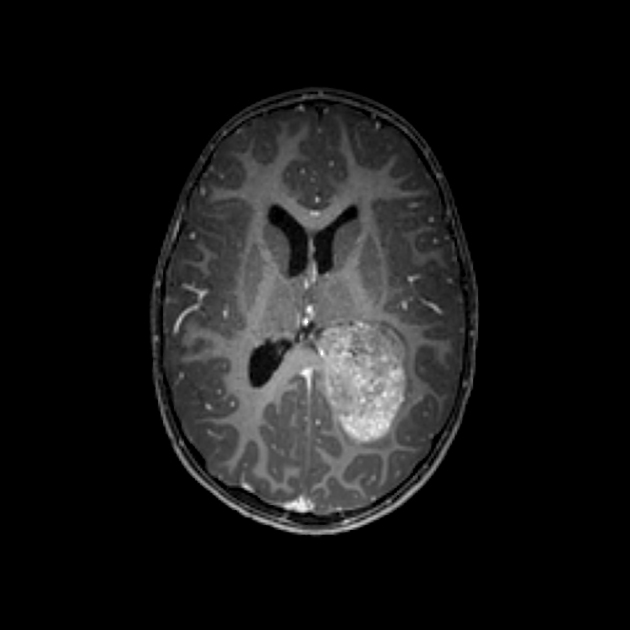
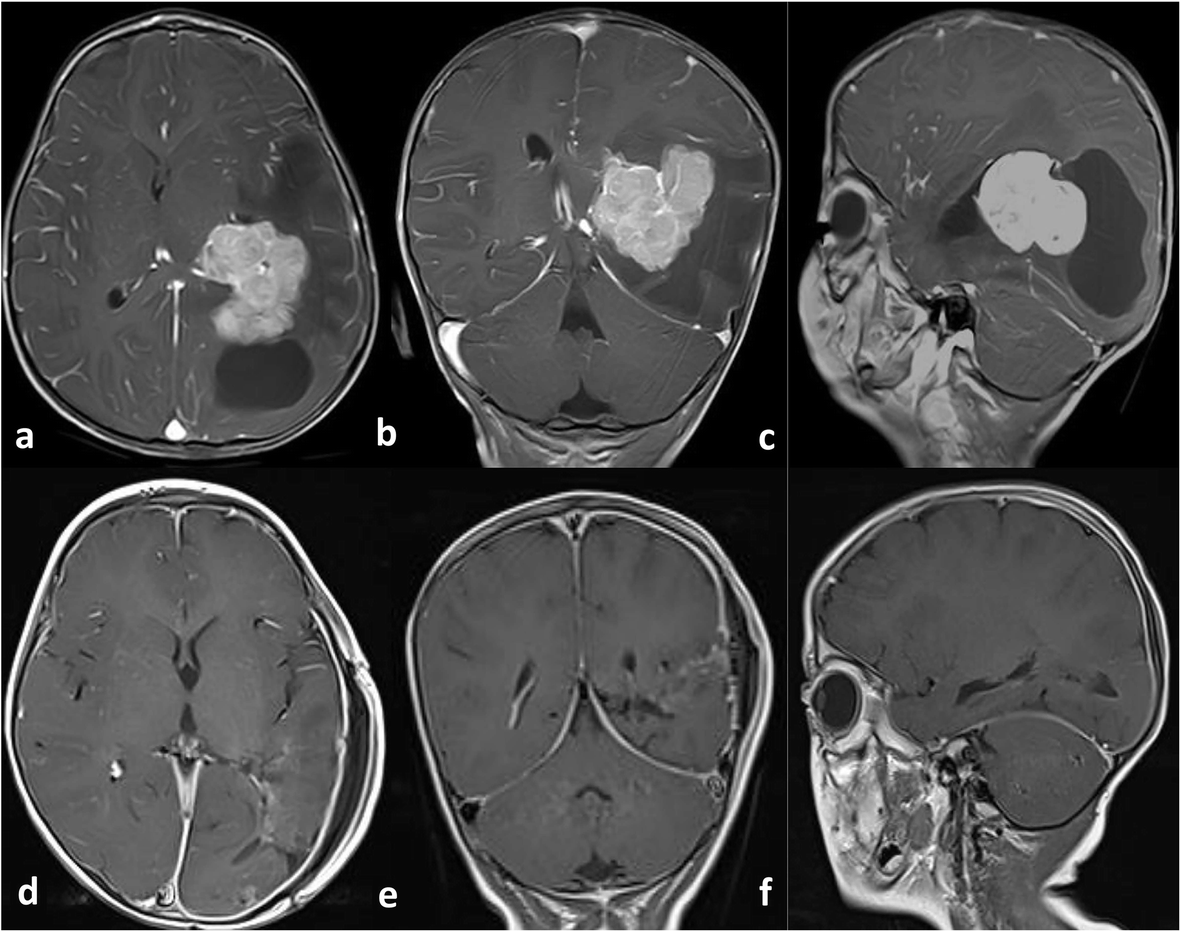
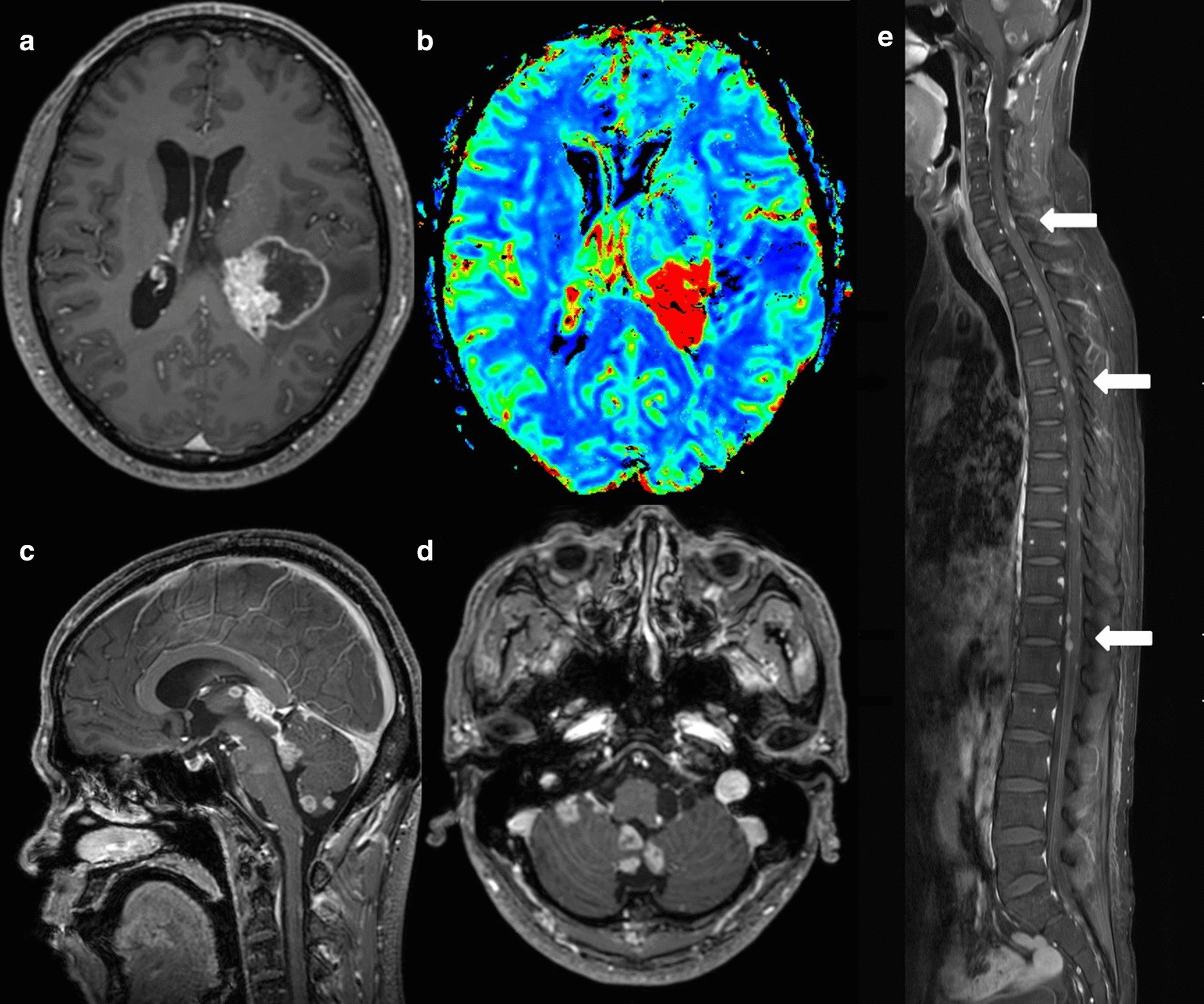
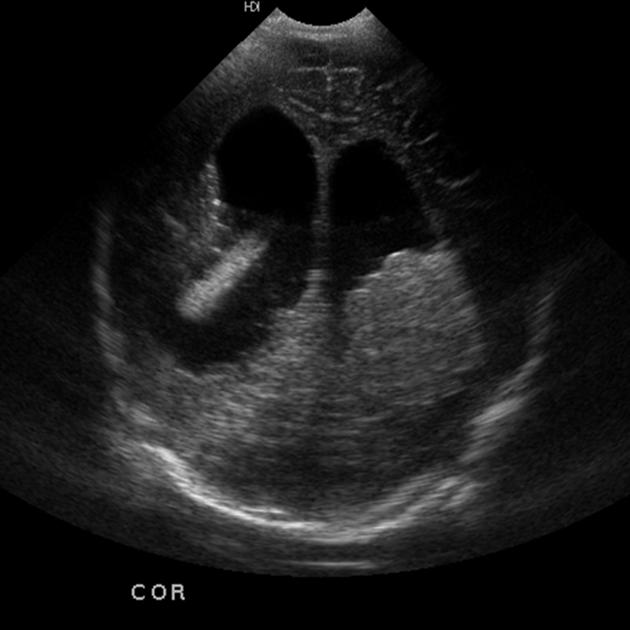
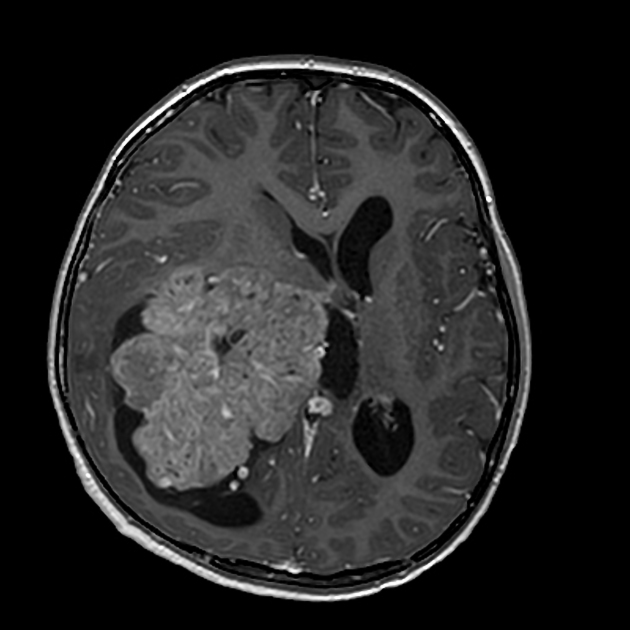
Choroid plexus carcinomas are markedly enhancing intraventricular tumors, usually arising in the trigone of a lateral ventricle and invading adjacent brain parenchyma.
Hydrocephalus may be present but is less likely than with choroid plexus papillomas. In choroid plexus carcinomas, hydrocephalus is generally a consequence of mechanical CSF pathway obstruction by the mass or CSF seeding, whereas, in choroid plexus papillomas, there is at least a component of CSF overproduction.
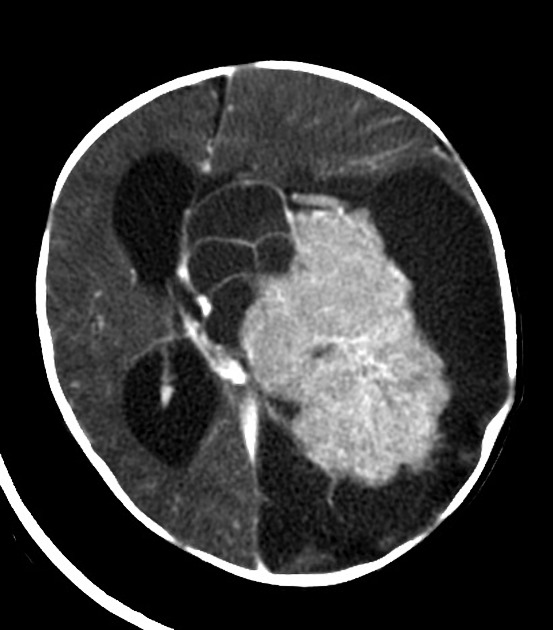
CT
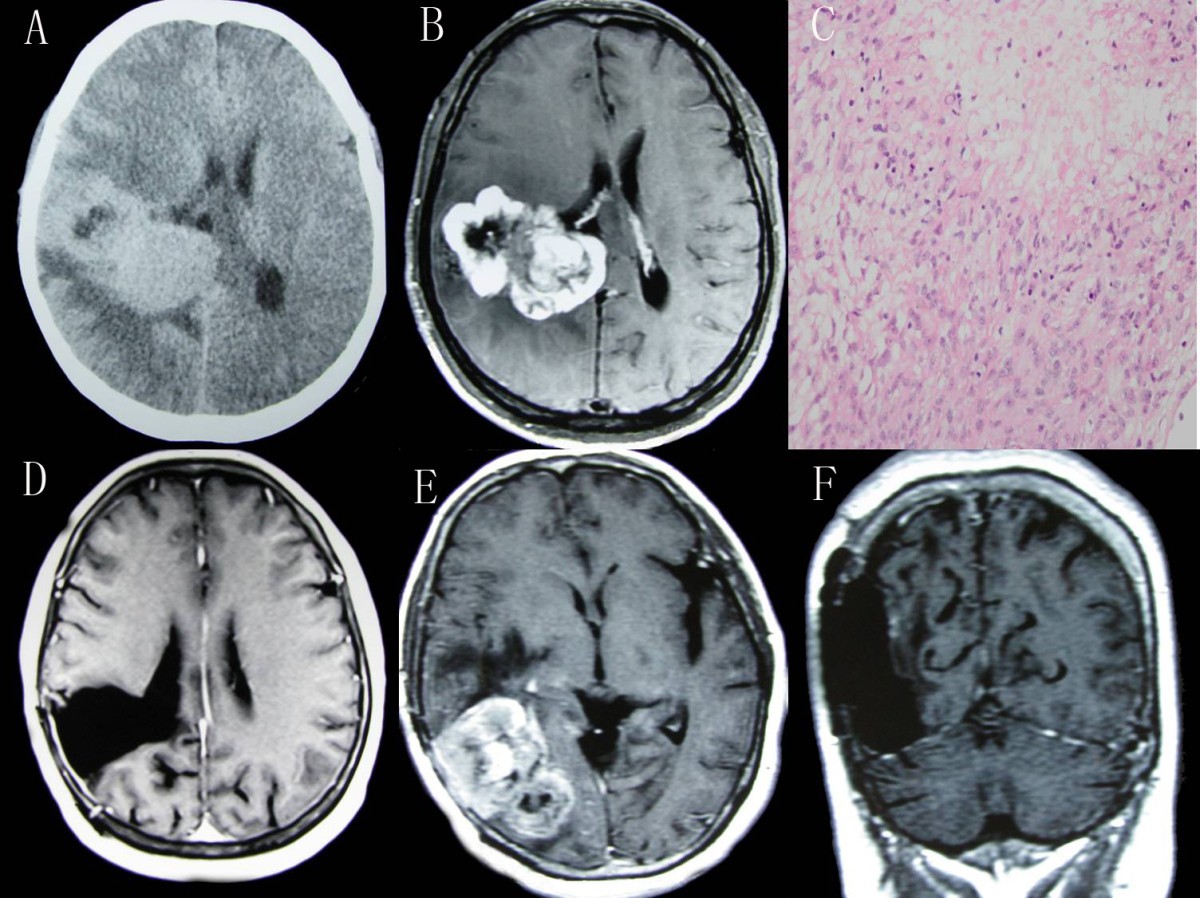
On non-contrast CT choroid plexus carcinomas are heterogeneous and typically iso to hyperdense to grey matter. Calcification may be seen in 20-25% of cases.
Contrast enhancement is usually prominent but heterogeneous with areas of necrosis and cyst formation evident.
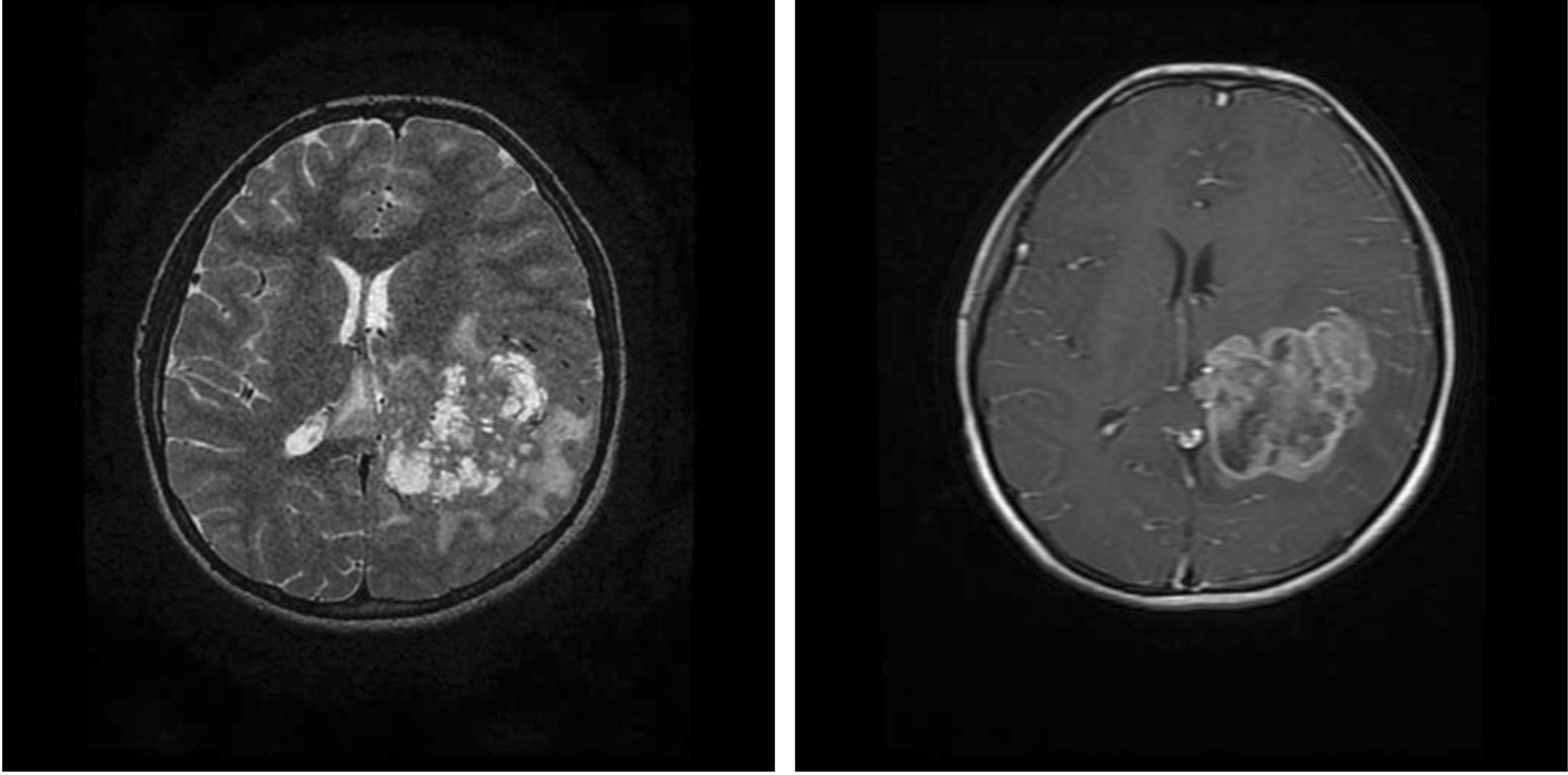
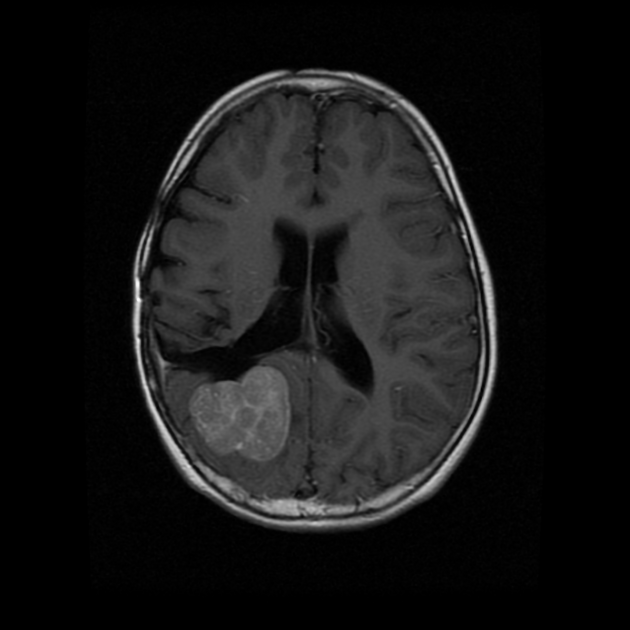
MRI
Reported signal characteristics include
- T1: iso- to hypointense
- T2: iso- to hypointense with hyperintense necrotic areas
- T2* GRE: blooming from calcifications/hemorrhage
- T1 C+ (Gd): can show marked, heterogeneous enhancement.
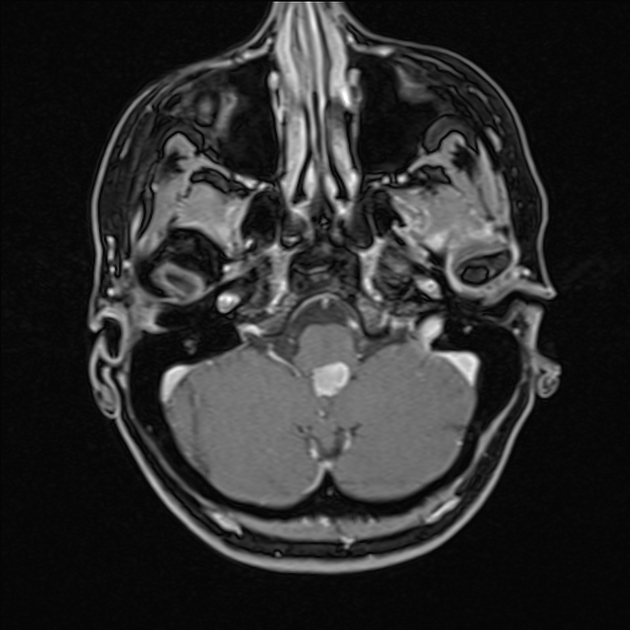
The tumors may have CSF seeding, therefore imaging of the entire neural axis is recommended prior to surgery.
Treatment and prognosis
Choroid plexus carcinomas are rapidly growing tumors with a 40% 5-year survival. TP53 mutation, brain invasion and CSF seeding are considered poor prognostic factors .
Surgical en-bloc resection is the mainstay of treatment and can result in a cure, achieved in as many as 50% of cases, but this result has only been reported in some selected series . In general, survival seems to be much worse than this, and hinges upon the ability to achieve gross complete macroscopic resection. In such cases, a 5-year survival of up to 86% can be achieved. In cases where resection is incomplete, 5-year survival is much lower 26% . Both radiotherapy and chemotherapy are used .
Differential diagnosis
General imaging differential considerations include:
- choroid plexus papilloma and atypical choroid plexus papilloma
- generally difficult to categorically distinguish these on imaging alone, however some features are helpful:
- homogeneous
- lack of necrosis
- lack of cerebral parenchymal invasion
- older age favors choroid plexus papilloma
- generally difficult to categorically distinguish these on imaging alone, however some features are helpful:
- central neurocytoma
- older demographic
- usually in the body of the lateral ventricle, typically abutting the septum pellucidum
- intraventricular meningioma
- older demographic
- more homogeneous outline and contrast enhancement
- choroid plexus metastasis
- rare in children
Further differentials to be considered in a large tumor, where the intraventricular origin may be difficult to ascertain, include PNET and GBM.
See also
- intraventricular masses (differential)
- intraventricular masses - an approach
Siehe auch:
- Glioblastoma multiforme
- intraventrikuläre Neoplasien und Läsionen
- Plexuspapillom
- intraventrikuläres Meningeom
- intraventrikuläre Neoplasien und Läsionen - Überblick
- intraventrikuläres Neurozytom
- Tumoren des Plexus choroideus
- Primitiver neuroektodermaler Tumor
- atypisches Plexuspapillom
- choroid plexus metastasis
und weiter:


 Assoziationen und Differentialdiagnosen zu Karzinom des Plexus choroideus:
Assoziationen und Differentialdiagnosen zu Karzinom des Plexus choroideus: