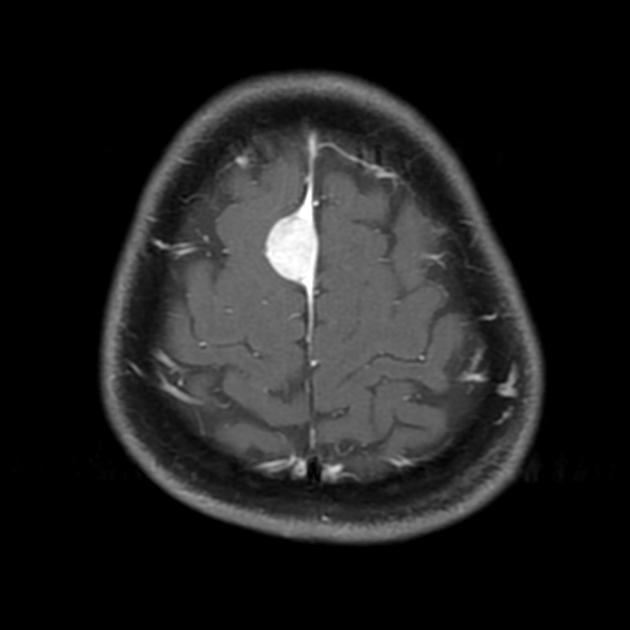
cystic meningiomas









The term cystic meningioma is applied to both meningiomas with intratumoral degenerative cyst formation as well as those with peritumoral arachnoid cysts or reactive intraparenchymal cysts.
They should not be confused with microcystic meningiomas, a distinct variant, in which the cysts are microscopic.
Epidemiology
True cystic meningiomas (type 1 and 2 - see below) are those with a few large central cysts and are uncommon. Those with more numerous smaller peripheral cysts are more frequent (8-23% of cases). They are over-represented in male patients and the pediatric population .
Clinical presentation
Patients present clinically in the same way as patients with non-cystic meningiomas, with either symptom related to increased intracranial pressure (ICP), focal neurology, or seizures.
Pathology
Various mechanisms have been proposed, and probably more than one is applicable depending on the location of the cysts:
- degeneration or necrosis
- direct secretion by meningioma
- reactive changes (peripheral arachnoid cysts)
Classification
This classification was initially proposed by Nauta et al. in 1979, which was later modified by Worthington et al. in 1985, which at the time of writing (July 2016) is most widely used classification.
Nauta et al. divided cystic meningiomas into four subtypes according to the location of the cyst with respect to the brain and meningioma :
- type 1: intratumoral cyst(s), located centrally within the meningioma
- type 2: intratumoral cyst(s), situated peripherally within the meningioma but still surrounded by tumor
- type 3: cyst wall may contain nest of tumor cells.
- type 4: cyst(s) located within the adjacent brain
- type 5: cyst(s) located between the meningioma and brain (arachnoid cyst)
4th type is most common.
Radiographic features
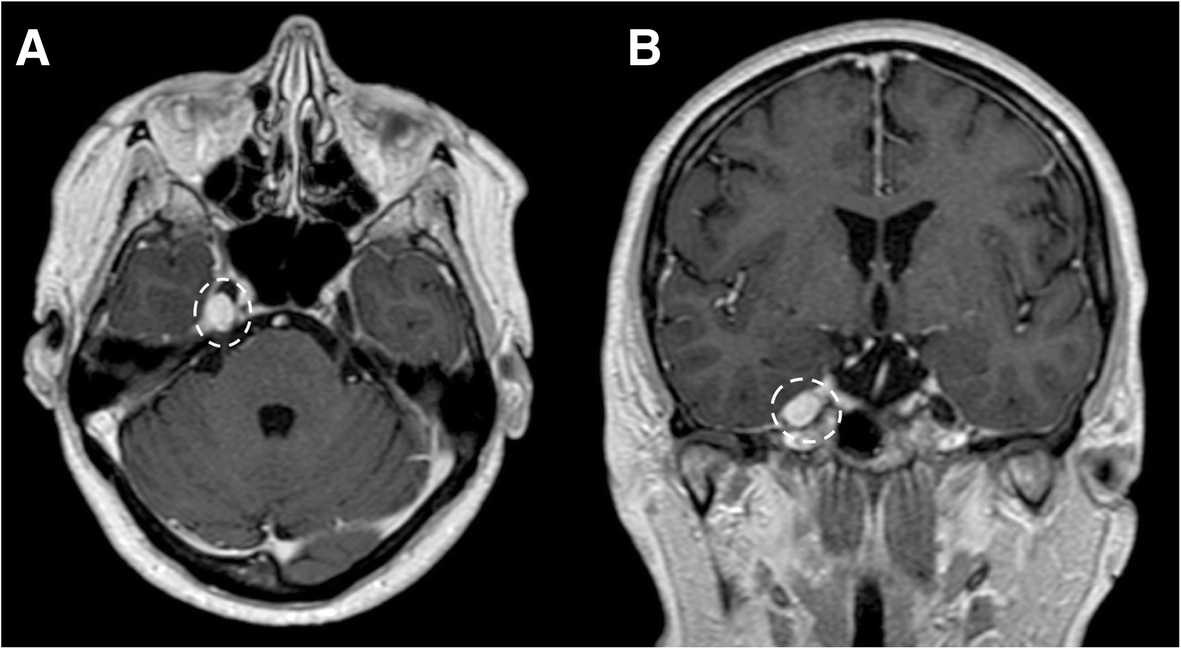
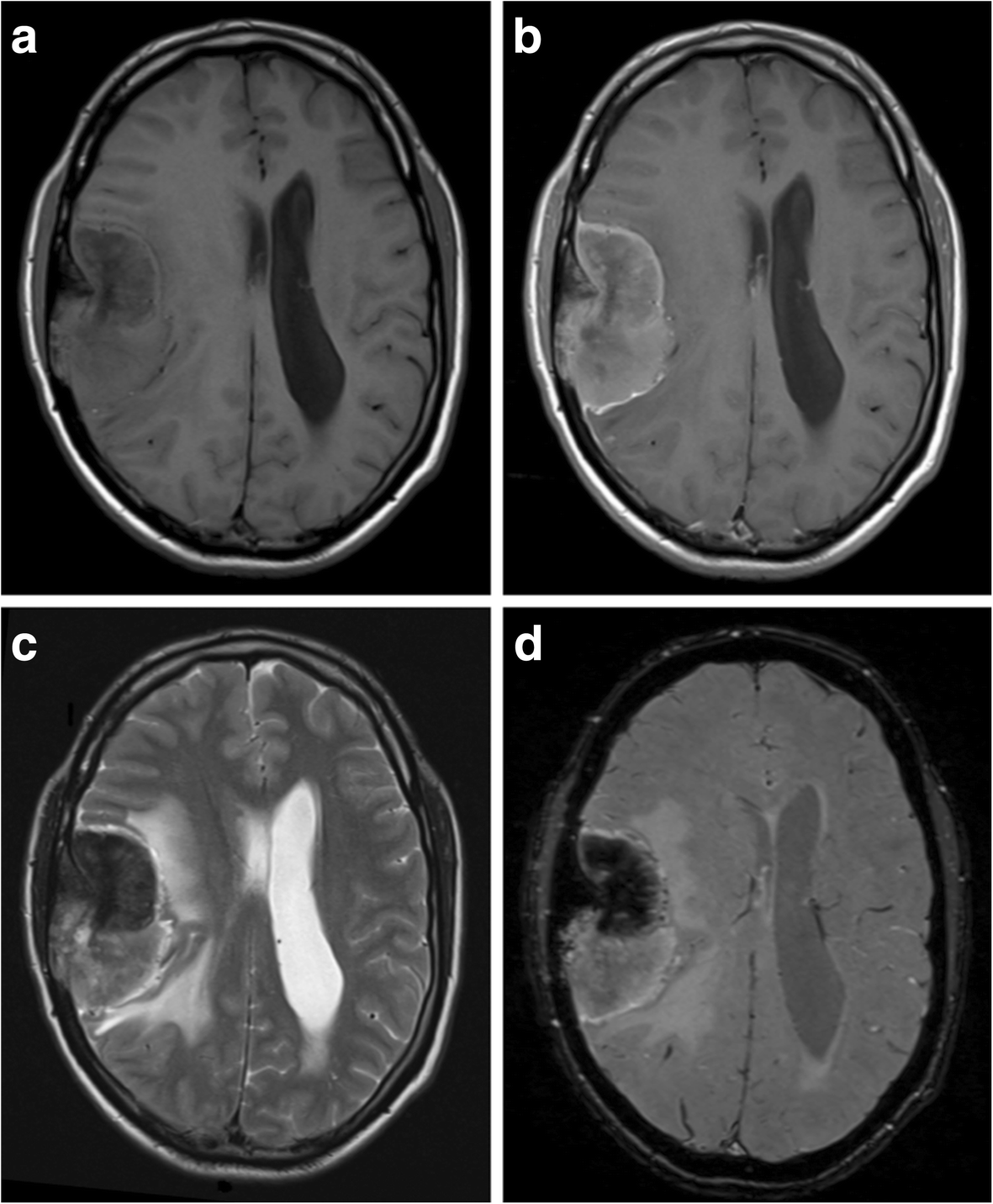
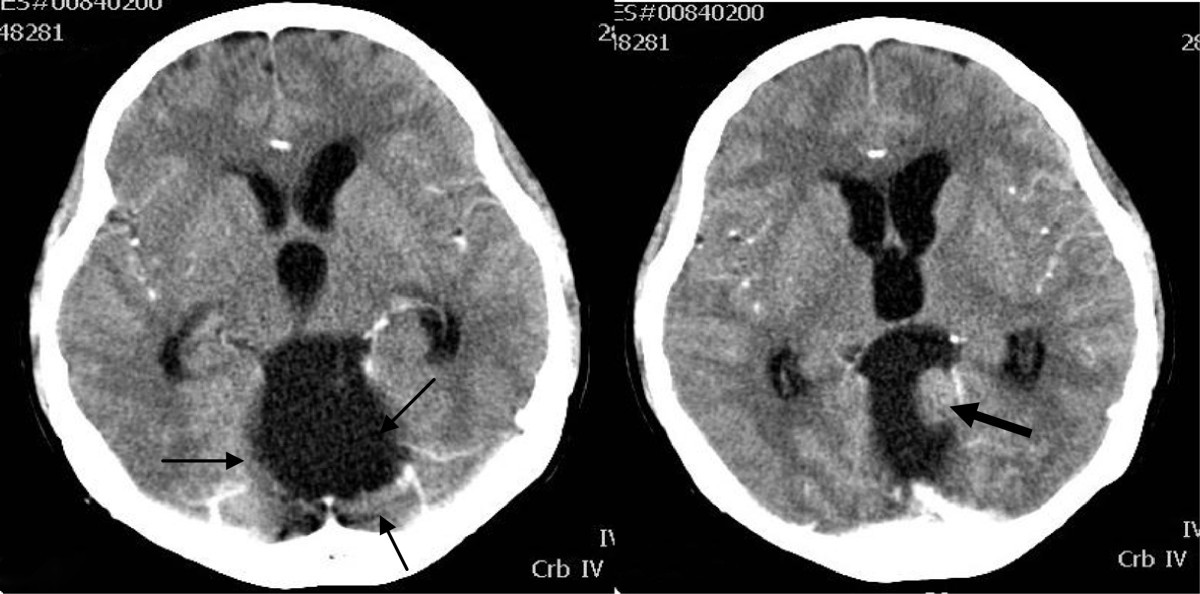
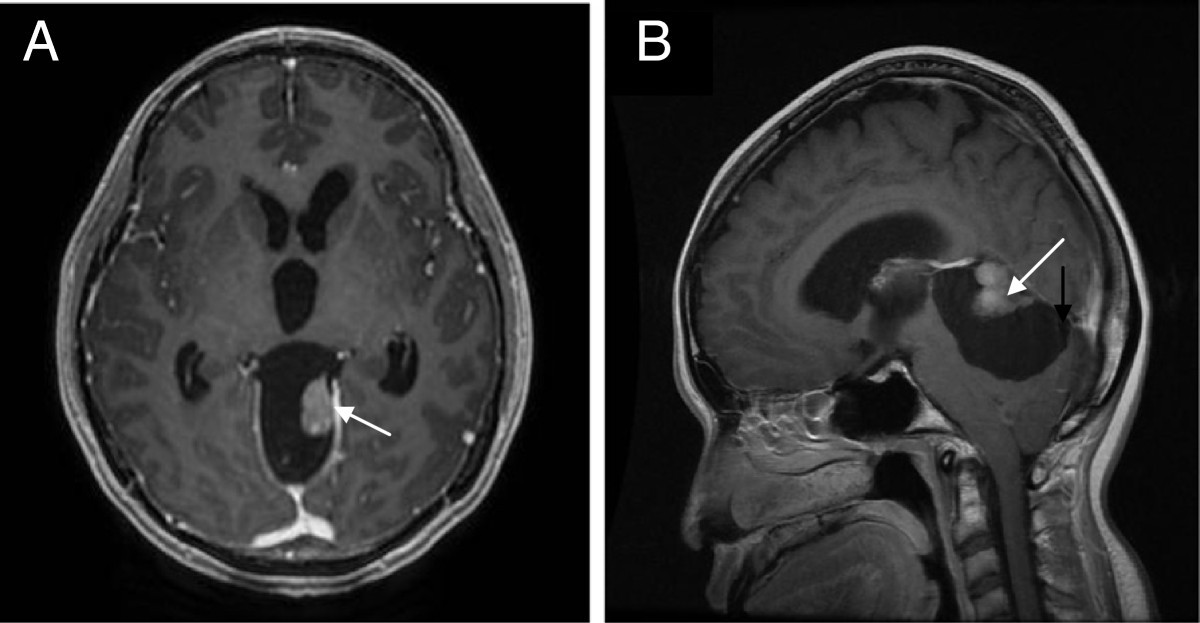
The tumor itself has imaging features identical to non-cystic meningiomas (see the meningioma main article for a full discussion). The cysts are of variable size and can be entirely surrounded by tumor (types 1 or 2) or clearly between the tumor and the brain (type 5) or within the adjacent brain (type 4). On imaging, it is sometimes difficult to distinguish between these types.
Differential diagnosis
The differential is dependent on the location of the tumor. For tumors around the base of the skull, cystic schwannomas (e.g. vestibular schwannoma, trigeminal schwannoma) are the main differential, as they share the bright contrast enhancement, and are commonly cystic when large.
Siehe auch:
- Meningeom
- trigeminal schwannoma
- atypical meningioma
- Vestibularisschwannom
- mikrozystisches Meningeom
- cystic extraaxial mass
und weiter:


 Assoziationen und Differentialdiagnosen zu cystic meningioma:
Assoziationen und Differentialdiagnosen zu cystic meningioma: