femoroazetabuläres Impingement (Pincertyp)



Pincer morphology refers to an abnormality of the acetabulum or rather an acetabular overcoverage of the femoral head, which may be focal or global, and is one of the causes of femoroacetabular impingement.
Terminology
Pincer morphology is also commonly referred to as 'pincer deformity', though according to the Warwick agreement ‘pincer morphology’ is the preferred term .
Epidemiology
Pincer morphology as an isolated finding does is not a very frequent cause of impingement and if symptomatic, it is usually found with coexisting cam morphology . It is most often found in middle-aged women.
Associations
Clinical presentation
Pincer morphology can be asymptomatic or if coupled with femoroacetabular impingement present with symptoms, for example, movement-related hip pain or groin pain and is then referred to as femoroacetabular impingement . Patients can also complain of decreased and painful range of motion.
Complications
The pincer deformity can lead to the following :
- labral tears particularly in the anterosuperior aspect of the acetabulum
- chondral damage, especially posteroinferiorly
- osteoarthritis of the hip
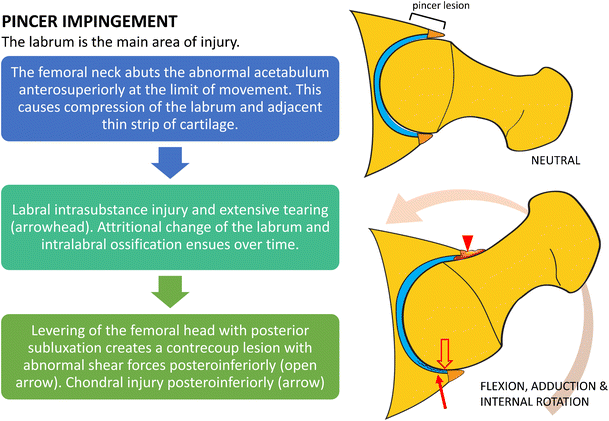
Pathology
Acetabular overcoverage is due to an increased acetabular depth such as coxa profunda or protrusio acetabuli, if focal it can be due to acetabular retroversion, a prominent posterior rim or an acetabular ossicle . Thus the anterior or anterosuperior acetabular rim usually builds up contact to the femoral neck, with possible associated symptoms and further development of a chondral contrecoup lesion typically found posteroinferiorly .
Etiology
The following conditions are considered etiologic factors of pincer-morphology :
- coxa profunda
- protrusio acetabuli
- posttraumatic acetabular deformity
- iatrogenic
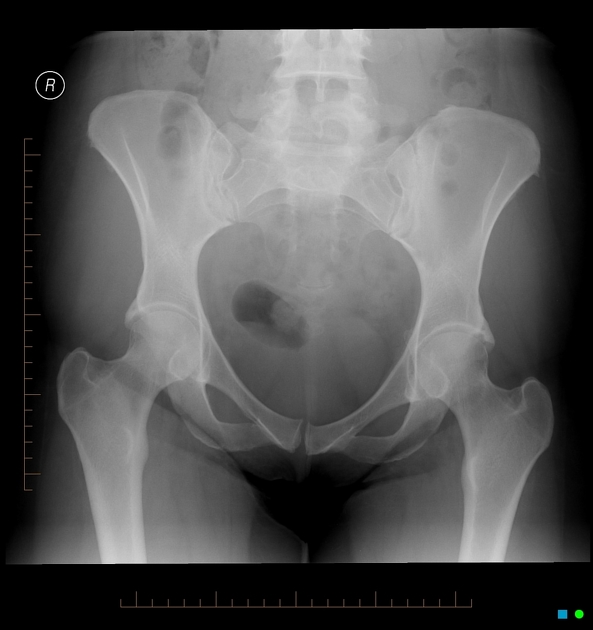
Radiographic features
AP view of the pelvis and a lateral femoral neck view is recommended for the initial evaluation . Cross-sectional imaging is recommended for the detection of chondral and labral lesions and preoperative planning .
Plain radiograph
Radiographic measures of pincer morphology include the following :
- ilioischial line for assessment of coxa profunda
- increased lateral center-edge angle > 40°
- acetabular index
- crossover sign
- ischial spine sign
- posterior wall sign
CT
The following morphological abnormalities can be assessed in addition 3D reconstructions enable surgical planning e.g. for osteochondroplasty :
- increased acetabular depth: the distance between the femoral head center and a line between the anterior and posterior acetabular rim on oblique axial images (anterior position)
- acetabular retroversion
- detection of an acetabular ossicle
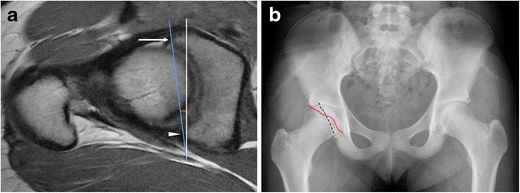
MRI
The following features can be assessed :
- increased acetabular depth: the distance between the femoral head center and a line between the anterior and posterior acetabular rim on oblique axial images (anterior position)
- acetabular retroversion
- labral tears and fissuring, especially anterosuperiorly
- chondral lesions (sensitivity and specificity is 59% and 94%) especially posteroinferiorly
MR arthrography
MR arthrography features a higher sensitivity for labral tears.
Radiological reporting
A report for preoperative should include the following :
- acetabular depth: coxa profunda, protusio acetabuli
- acetabular retroversion
- possible co-existing cam morphology
- labral damage and tears or labral ossification
- cartilage defects and lesions
- signs of early osteoarthritis: subchondral sclerosis, cysts, osteophytes
- associated soft tissue injuries: musculotendinous injury
Treatment and prognosis
Pincer morphology itself if asymptomatic can be managed with preventive measures.
Symptomatic femoroacetabular-impingement with pincer morphology can be treated conservatively or surgically. Conservative treatment approaches include activity and/or lifestyle modifications, physiotherapy, watchful waiting. Surgical treatment includes acetabular rim reconstruction or resection of the acetabular ossicle . Global acetabular over coverage, if symptomatic, should be approached more cautiously with arthroscopy and might be better treated with osteotomy .
However, surgical treatment should be only considered or performed if the whole triad of clinical signs, symptoms and morphological changes are present .
See also
Siehe auch:
- Femoro-acetabuläres Impingement
- Arthrose
- femoroacetabulares Impingement vom Cam-Typ
- cross-over sign Hüfte
- ventral impingement of the hip
und weiter:


 Assoziationen und Differentialdiagnosen zu femoroazetabuläres Impingement (Pincertyp):
Assoziationen und Differentialdiagnosen zu femoroazetabuläres Impingement (Pincertyp):