Humerusschaftfraktur


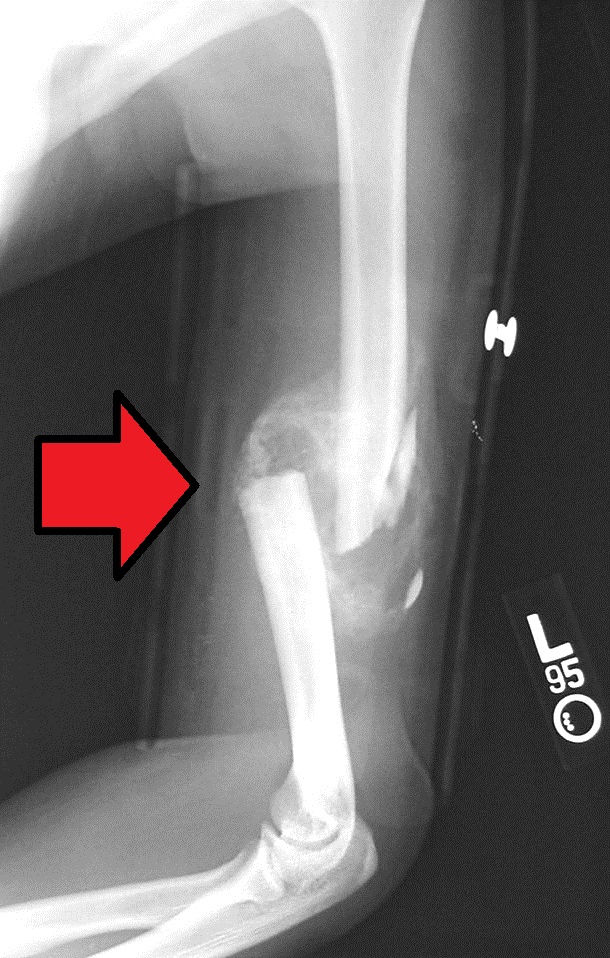


Humeral shaft fractures are readily diagnosed and usually, do not require internal fixation.
Epidemiology
Humeral shaft fractures account for 3-5% of all fractures . Although they occur in all age groups, a bimodal distribution is noted. The first peak is seen in the third decade in males and the second peak in the seventh decade in females .
Pathology
Mechanism
Most frequently humeral shaft fractures occur as a result of a direct blow to the upper arm (transverse fractures). Indirect trauma from a fall or a twisting action (e.g. arm wrestling) are also encountered and usually result in spiral or oblique fractures . The higher the impact strength, the more likely the fracture is to be comminuted . A minority are open fractures (2-10%) .
The most common associated injury is damage to the radial nerve, on account of its very close relationship to the posterior aspect of the bone, running in the spiral groove between the lateral and medial heads of the triceps muscle. .
Damage to the brachial artery, median and ulnar nerves are much less common.
Radiographic features
Fractures are unevenly distributed along the humeral diaphysis :
- proximal third: 30%
- middle third: 60%
- distal third: 10%
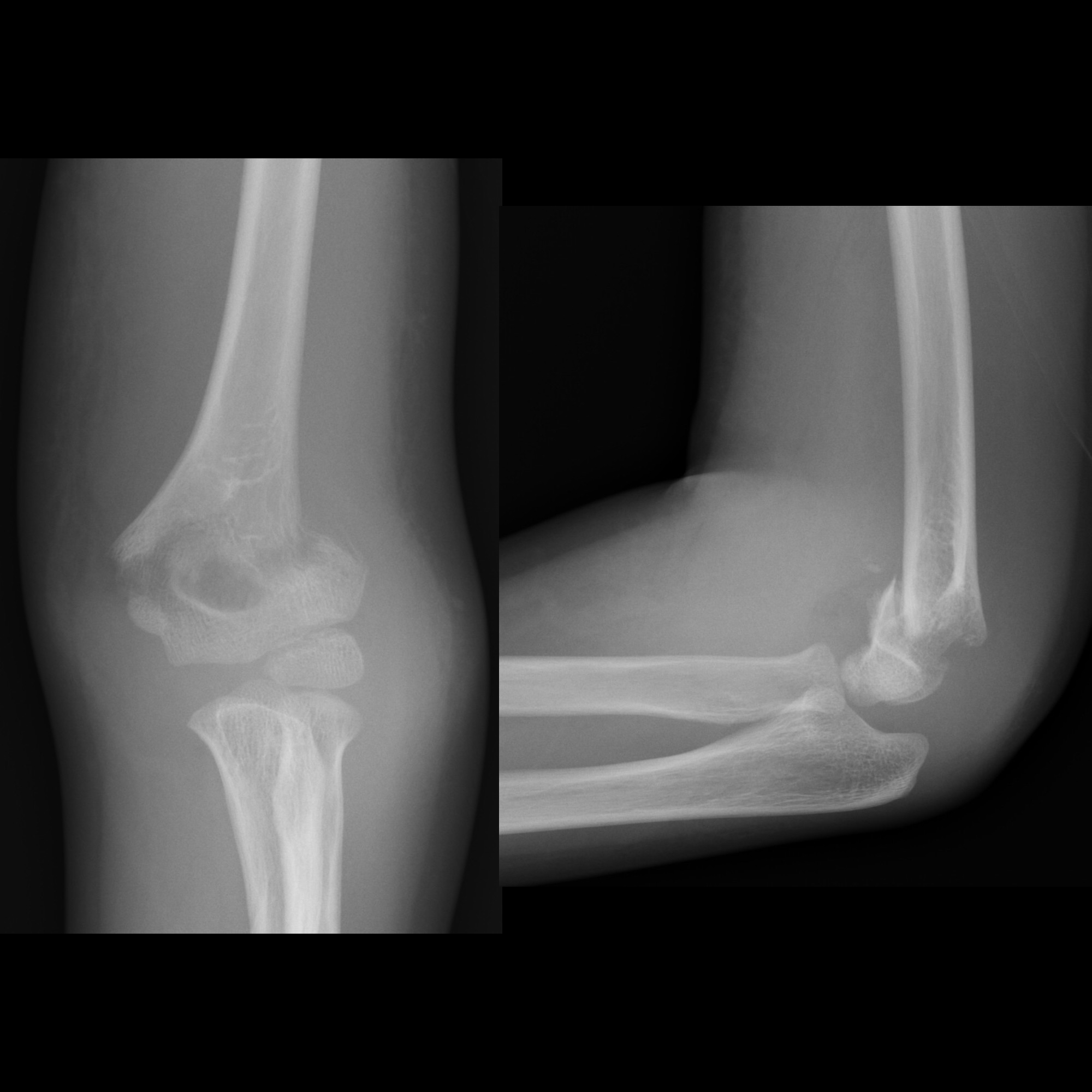
Plain radiography
Although transverse fractures are usually trivially easy to identify, oblique or spiral fractures can be very difficult to identify in a single view. The radiographic series comprises an AP and a lateral projection to allow adequate assessment of angulation, displacement and shortening . It is essential both the shoulder joint and the elbow joint are included to assess for proximal or distal extension of the fracture.
Report checklist
In addition to reporting on the presence of a fracture, a number of features should be assessed and commented on:
- fracture
- location and extension to metaphysis/epiphysis/articular surface
- type of fracture (transverse, spiral, oblique)
- comminution/segmental
- angulation, displacement and shortening
- open vs. closed; gas in soft tissues or foreign bodies
- underlying bony lesions (i.e. pathological fractures)
- carefully assess the elbow and shoulder for secondary injuries (be careful, as these will be sub-optimally imaged unless dedicated views are obtained)
Treatment and prognosis
Humeral shaft fractures are usually treated with a supportive/hanging cast followed by a supportive splint and infrequently require open reduction. Although anatomical reduction is not easily achieved, significant angulation (20 degrees) can be tolerated with little functional impairment. Similarly, up to 3-5 cm of shortening is in many cases acceptable .
Open reduction - internal fixation (ORIF) is required in a number of scenarios, including :
- adequate alignment cannot be maintained (more commonly encountered in transverse fractures)
- open fractures
- presence of vascular injury
- segmental fracture
- floating elbow
- presence of significant other injuries (poly-trauma, brachial plexus injury)
- non-union
- pathological fracture
In many instances presence of radial nerve palsy is not an indication for exploration, with the majority of patients recovering radial nerve function within 3-6 months . The role of open reduction and internal fixation in this situation is controversial .
The non-union rates for fractures managed non-operatively are low, only ~4% .
See also
Siehe auch:
- proximale Humerusfrakturen
- suprakondyläre Humerusfrakturen
- Frakturen der oberen Extremitäten
- Humerusfraktur
- Armdrückerfraktur
- Holstein-Lewis-Fraktur
und weiter:


 Assoziationen und Differentialdiagnosen zu Humerusschaftfraktur:
Assoziationen und Differentialdiagnosen zu Humerusschaftfraktur: