medial epicondyle fracture









Medial epicondyle fractures represent almost all epicondyle fractures and occur when there is avulsion of the medial epicondyle. They are typically seen in children, and can be challenging to identify. Failure to diagnose these injuries can lead to significant long term disability.
Epidemiology
Medial epicondylar avulsion fractures are the most common avulsion injury of the elbow and are typically seen in children and adolescents .
Mechanism
A number of mechanisms have been implicated in medial epicondylar avulsion fractures :
- posterior elbow dislocation transmitting force to the medial epicondyle via the ulnar collateral ligament (most common; accounts for two thirds of cases of medial epicondylar fractures )
- fall on an outstretched hand with the elbow in full extension, resulting in sudden traction on the flexor pronator muscle group of the forearm
- direct blow (rare)
- chronic injury can also occur both in children (little league elbow) and adults (golfer's elbow) - discussed separately
Radiographic features
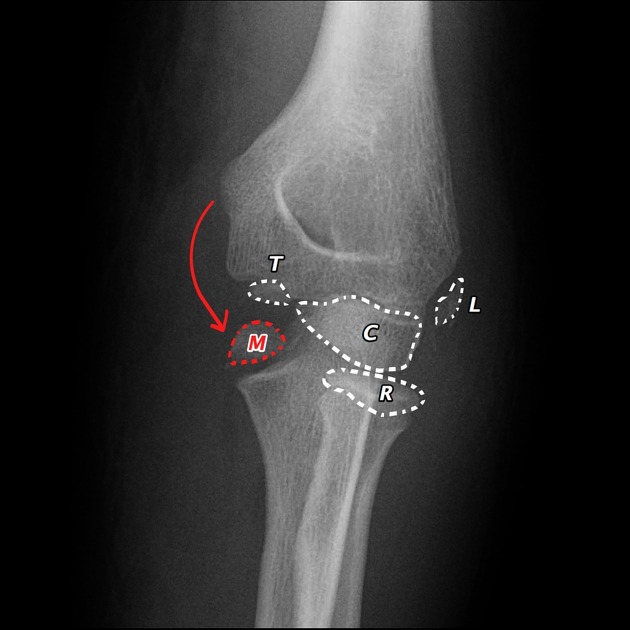
In young patients, knowledge of the sequence of ossification of the elbow (remembered using the mnemonic CRITOE) is essential as an avulsed and displaced apophysis can mimic another center.
Overall all centers are ossified by approximately 12 years of age, appearing in a predictable order: capitellum, radial head, medial (internal) epicondyle, trochlear, olecranon, and lastly lateral (external) epicondyle). Any missing ossification center or centers appearing in the wrong sequence should be viewed with a high suspicion of injury.
A particularly devastating miss is that of an avulsed fragment displaced into the joint, mimicking the center of ossification of the trochlear .
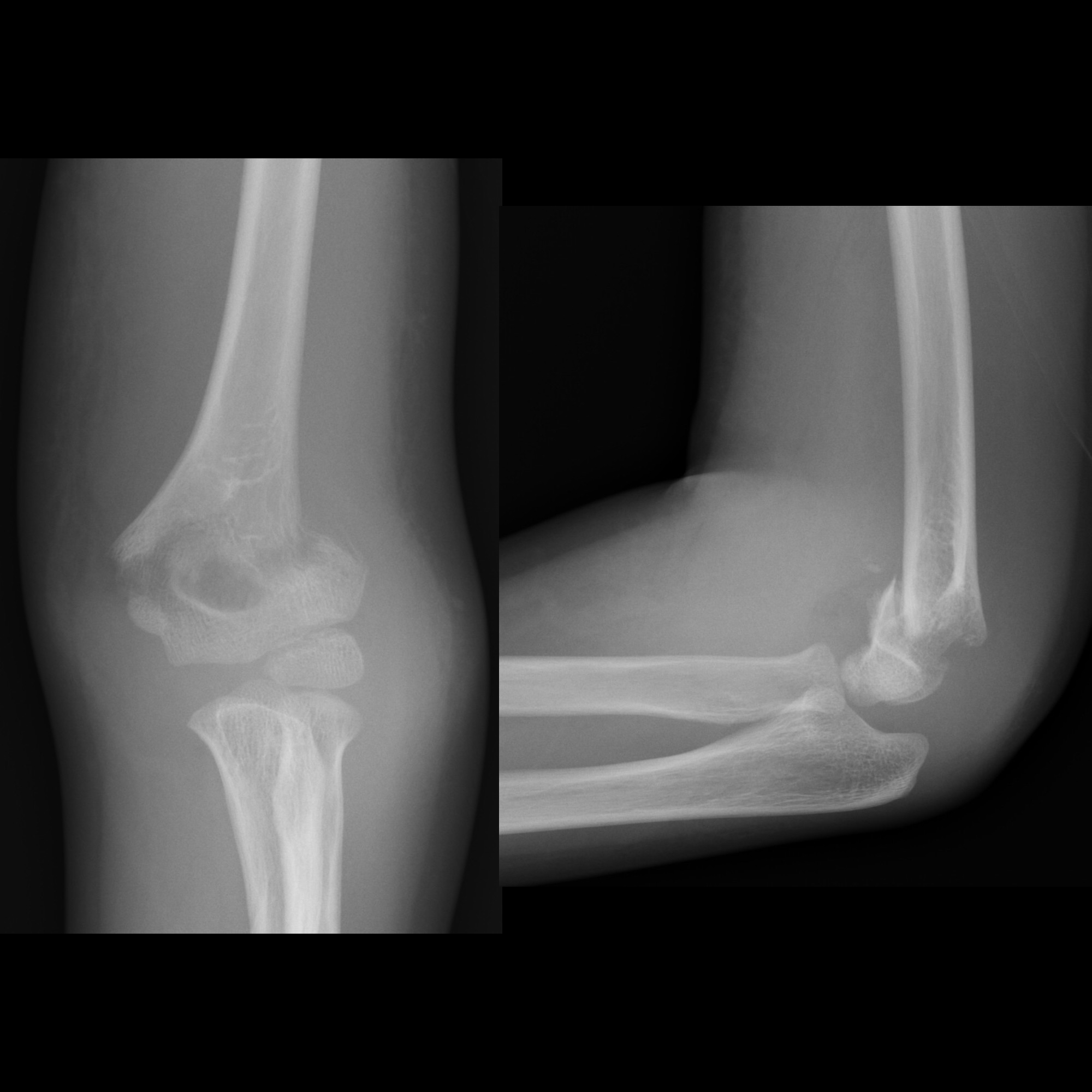
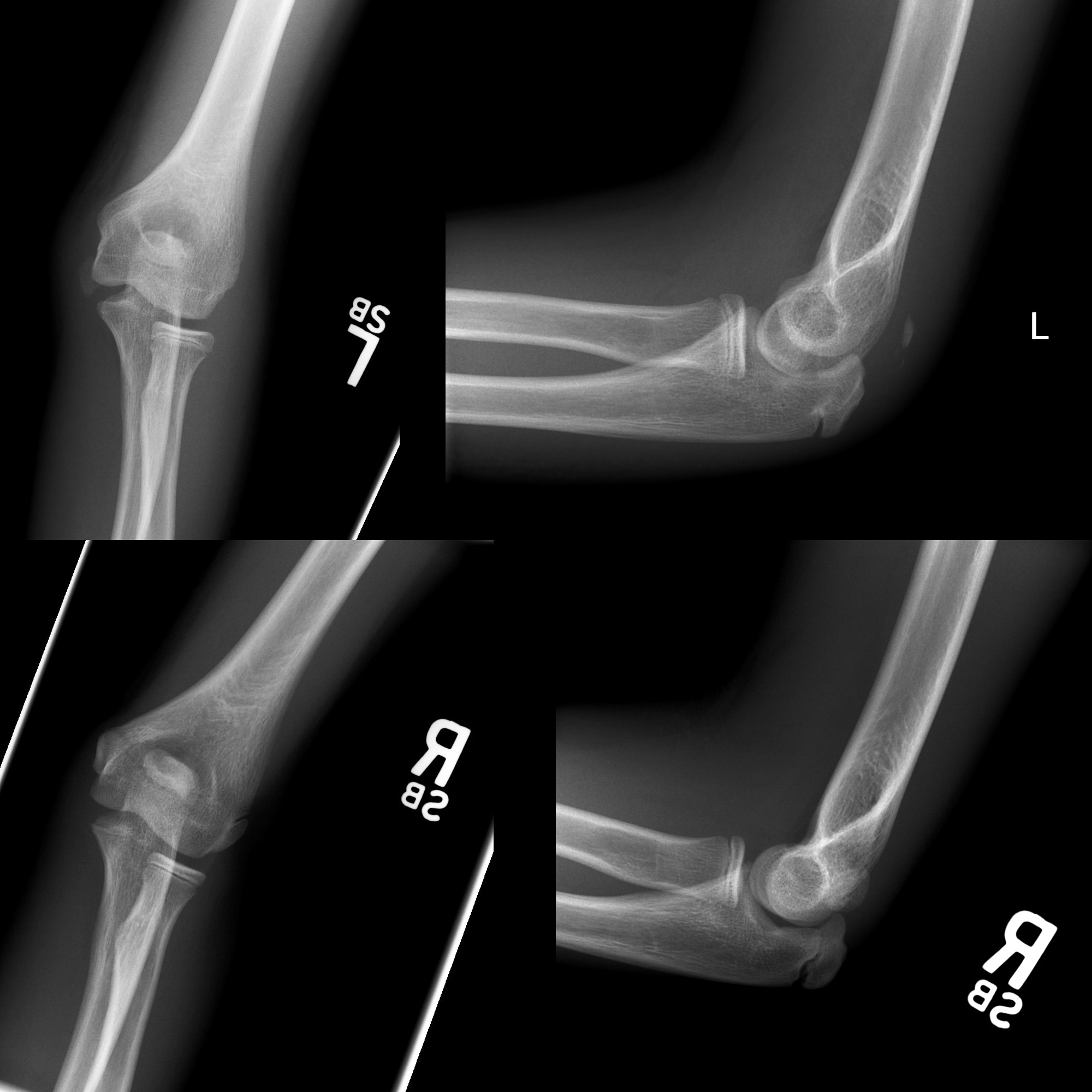
Plain radiograph
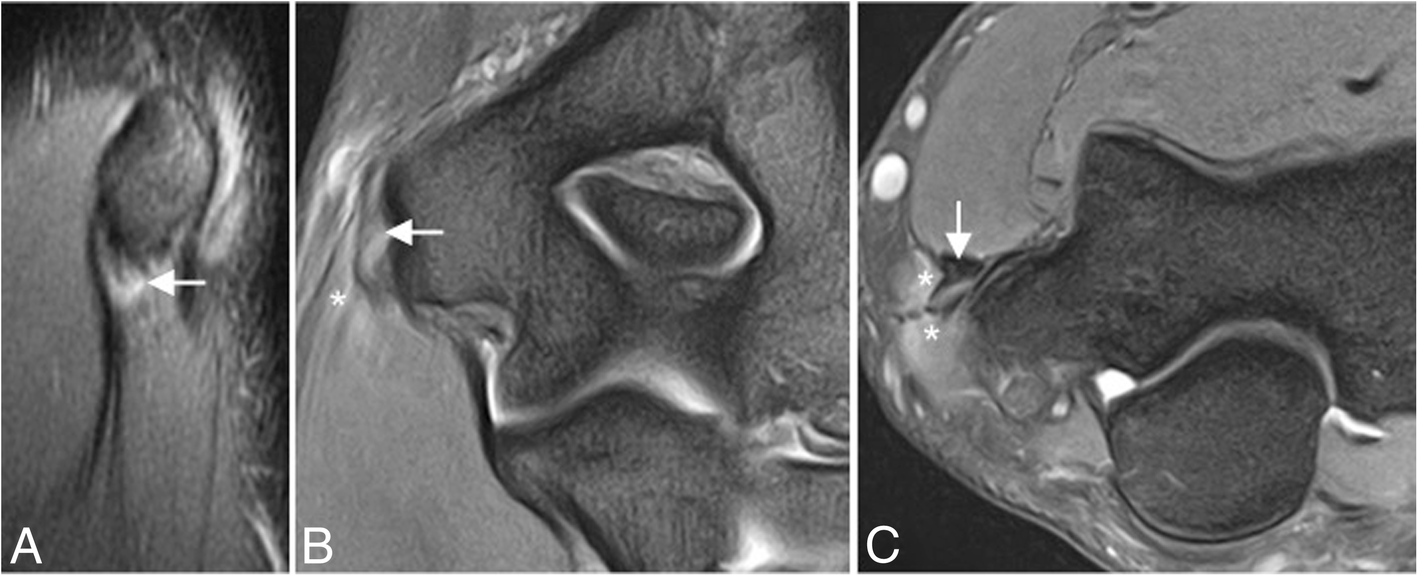
Plain films are usually sufficient for assessment of medial epicondylar avulsion fractures. If in doubt, comparison with the contralateral side can be helpful to diagnose a slight injury. In the setting of more complex injury, a cross-sectional imaging may be needed.
Features of a medial epicondylar avulsion injury include :
- soft tissue swelling
- this may be the only sign of an undisplaced injury
- this may be the only sign in children younger than ~7 years, in whom the medial apophysis is not ossified
- widening of the growth plate (comparison to the contralateral side may be useful)
- obvious displacement of the apophysis
- fracture through the adjacent humeral metaphysis
Radiology report
In addition to stating that a medial epicondylar fracture is present, a number of features should be sought and commented upon:
- avulsion
- degree of displacement
- location of the displaced fragment
- presence of a fracture of the adjacent humeral metaphysis
- presence of comminution of the apophysis
- elbow
- careful assessment of the centers of ossification to ensure they are age appropriate (see CRITOE)
- evidence of elbow dislocation (spontaneous reduction at the time of injury may have occurred)
- coronoid process and radial head fractures (terrible triad of the elbow)
Treatment and prognosis
Treatment depends on both the particulars of the fracture and the patient.
An undisplaced fracture, particularly in the non-dominant arm of a non-athlete can be treated conservatively (three weeks in an upper arm splint) with good results .
Minimally displaced fractures can be treated with either cast immobilization or an upper arm splint, with a 50% of resulting in a pseudoarthrosis .
Displaced fractures or those occurring in the dominant arm, especially in athletes, need operative management, typically with open reduction and internal fixation with a cannulated screw, which results in rigid fixation permitting early motion . Bony union is achieved in 90% of cases .
Comminuted fractures can also be treated by suture fixation .
Fortunately, as these injuries involve an apophysis rather than an epiphysis, no growth arrest of the arm occurs, however elbow instability and even recurrent dislocations can result from suboptimal healing .
Siehe auch:
- Ellenbogenluxation
- Ossifikationszentren Ellenbogen
- suprakondyläre Humerusfrakturen
- humeral condyle fracture
- terrible triad of the elbow
- Epicondylus radialis Fraktur
- epicondylar fracture
- Ellenbogenfraktur
- Epicondylitis ulnaris humeri
- CRITOE
- Epikondylusfrakturen am Ellenbogen
und weiter:


 Assoziationen und Differentialdiagnosen zu Abrissfraktur Epikondylus ulnaris:
Assoziationen und Differentialdiagnosen zu Abrissfraktur Epikondylus ulnaris: