pseudoachalasia










Pseudoachalasia (a.k.a. secondary achalasia) is an achalasia-pattern dilatation of the esophagus due to the narrowing of the distal esophagus from causes other than primary denervation. One of the most common causes is malignancy (often submucosal gastric cancer) with extension in the lower esophagus. The clinical and imaging similarities of achalasia and pseudoachalasia may pose a diagnostic challenge, usually requiring further investigation.
Clinical presentation
The clinical course of pseudoachalasia depends on the underlying cause however it, in particular, if secondary to the neoplasm, is usually short (<6 months) unlike the chronic clinical history in patients with primary achalasia. Patients also tend to be older (>50 years) than those with primary achalasia.
Pathology
Etiology
- esophageal malignancy
- gastric carcinoma (of the cardia and fundus)
- esophageal carcinoma
- lymphoma
- central and peripheral neuropathy
- brainstem stroke
- brainstem infiltration, e.g. malignancy, amyloidosis
- infiltration of vagus by malignancy
- complication of bilateral vagotomy
- chronic idiopathic intestinal pseudo-obstruction
- diabetes mellitus
- paraneoplastic
- esophageal stricture
- ischemia
- gastro-esophageal reflux
- acid/alkali ingestion
- scleroderma
- the patulous esophagus in some presentations of scleroderma may lead to chronic severe reflux and development of a distal esophageal stricture
- this patient population is also at risk for esophageal carcinoma
The pathophysiology of pseudoachalasia is thought to be twofold:
Although less common, it is possible for primary achalasia and malignancy to coexist.
Radiographic features
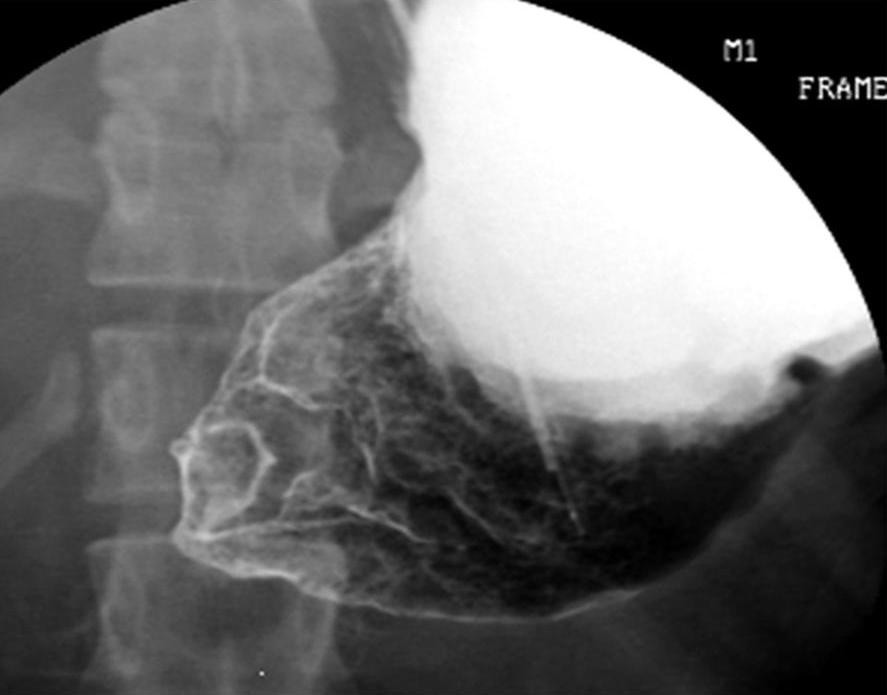
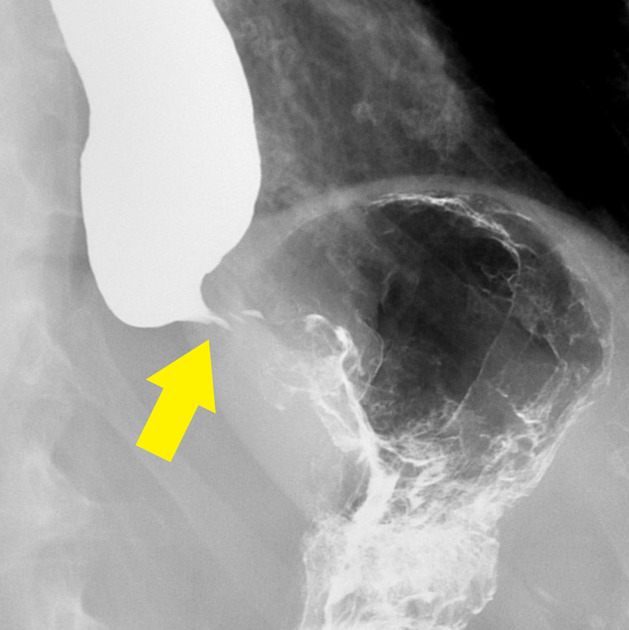
The plain chest film and barium swallow findings are similar to achalasia and may also show other features of the underlying cause (listed above).
Two useful discriminators in barium swallow, particularly in cases secondary to underlying neoplasm, are
- more marked mucosal irregularity of malignant lesions in pseudoachalasia
- the temporary patency of lower esophageal sphincter if the hydrostatic pressure is increased in achalasia
CT is usually the imaging modality of choice for equivocal cases because it more clearly depicts a malignant lesion, as well as potential lymph node involvement, local invasion, or metastatic spread.
Siehe auch:
- Ösophaguskarzinom
- prästenotische Dilatation
- Achalasie
- Amyloidose
- Adenokarzinom des Magens
- Systemische Sklerodermie
- Magen
- Ösophagusstrikur
und weiter:


 Assoziationen und Differentialdiagnosen zu Pseudoachalasie:
Assoziationen und Differentialdiagnosen zu Pseudoachalasie: