septal lines in lung





Septal lines, also known as Kerley lines, are seen when the interlobular septa in the pulmonary interstitium become prominent. This may be because of lymphatic engorgement or edema of the connective tissues of the interlobular septa. They usually occur when pulmonary capillary wedge pressure reaches 20-25 mmHg.
Classification
Kerley A lines
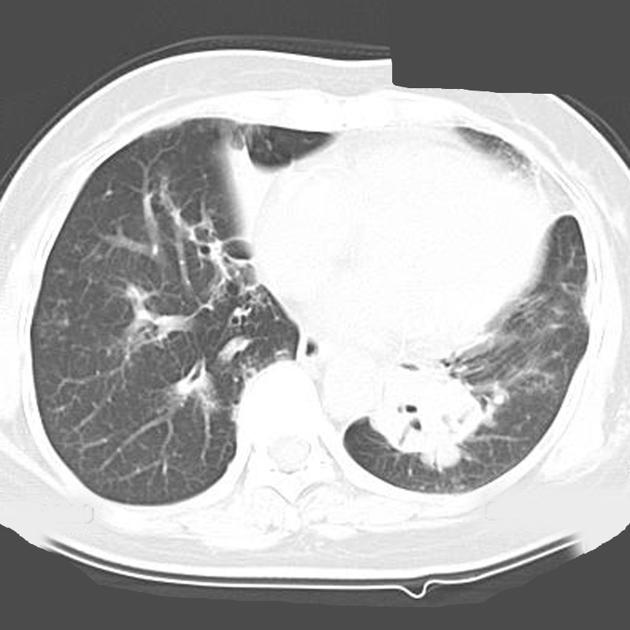
These are 2-6 cm long oblique lines that are <1 mm thick and course towards the hila. They represent thickening of the interlobular septa that contain lymphatic connections between the perivenous and bronchoarterial lymphatics deep within the lung parenchyma. On chest radiographs they are seen to cross normal vascular markings and extend radially from the hilum to the upper lobes. HRCT is the best modality for the demonstration of Kerley A lines.
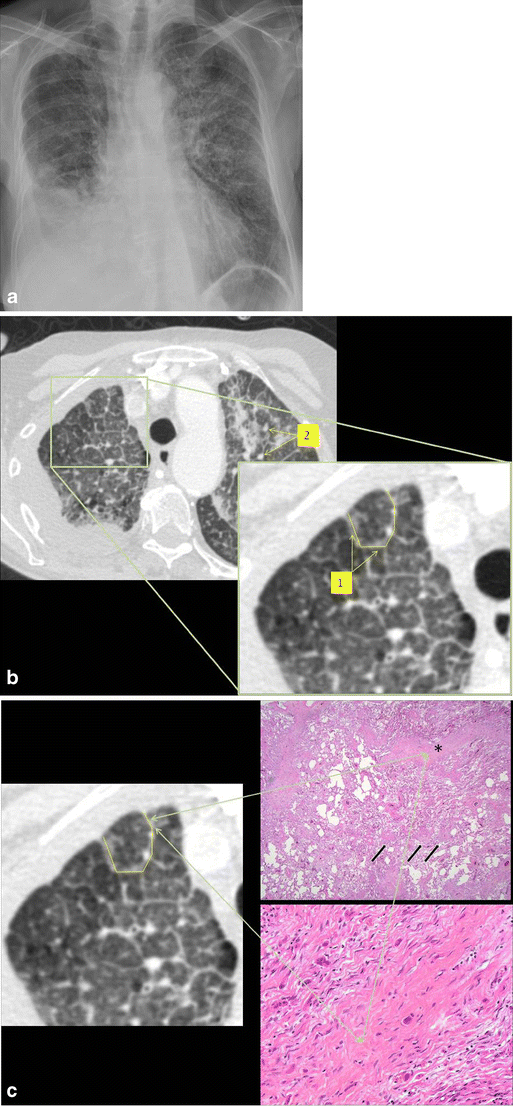
Kerley B lines
These are thin lines 1-2 cm in length in the periphery of the lung(s). They are perpendicular to the pleural surface and extend out to it. They represent thickened subpleural interlobular septa and are usually seen at the lung bases.
Kerley C lines
Kerley C lines are short lines which do not reach the pleura (i.e. not B or D lines) and do not course radially away from the hila (i.e. not A lines).
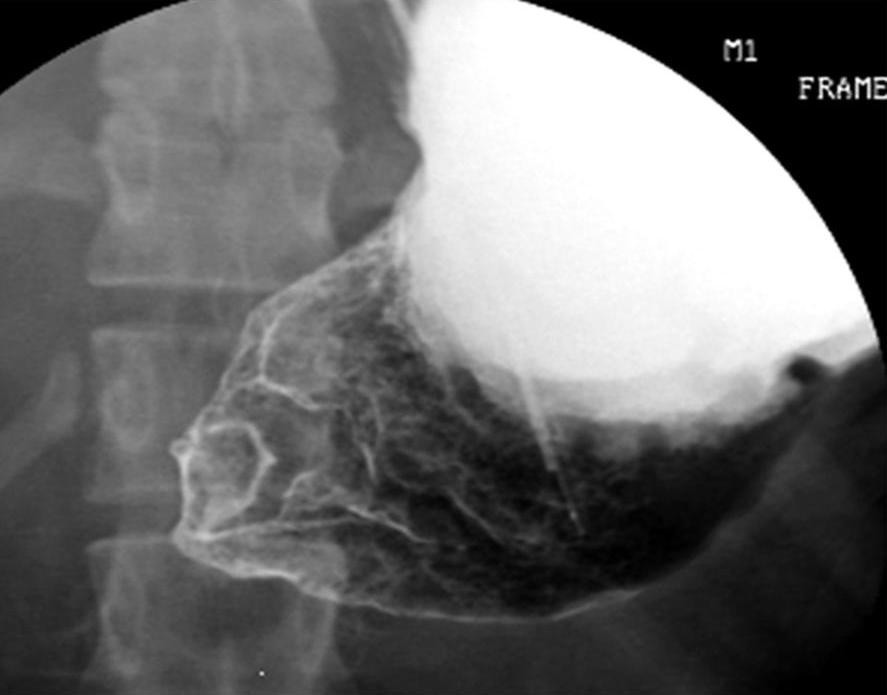
Kerley D lines
Kerley D lines are exactly the same as Kerley B lines, except that they are seen on lateral chest radiographs in the retrosternal air gap .
Pathology
Causes
- pulmonary edema
- neoplasm
- lymphangitic spread of cancer (e.g. lymphangitic carcinomatosis): Kerley lines with a fine peripheral reticular pattern
- lymphoma
- pneumonia
- interstitial pulmonary fibrosis
- pneumoconiosis
- sarcoidosis
History and etymology
Kerley lines are named after Sir Peter James Kerley (1900-1979), an Irish radiologist who in addition to describing the interstitial lines now known as Kerley lines, was a co-founder of the Faculty of Radiology (later to become the Royal College of Radiologists), and also attended to King George VI .
See also
- linear opacification
- linear interstitial pattern
Siehe auch:
- pulmonalvenöse Stauung
- Lungenödem
- Sarkoidose
- Kerley-Linien
- Lungenkarzinom
- Mammakarzinom
- Lymphangiosis carcinomatosa
- congestive heart failure
- Pankreaskarzinom
- Adenokarzinom des Magens
- Kerley-B-Linien
- Kerley-B-Linien
- Kolorektales Karzinom
- Pneumonokoniose
- Lymphom pulmonale Manifestation
- pulmonary interstitium
- Interlobulärseptum
- Kerley-C-Linien
- Pneumocystis jiroveci Pneumonie
- linear opacification
und weiter:


 Assoziationen und Differentialdiagnosen zu Kerley-B-Linien:
Assoziationen und Differentialdiagnosen zu Kerley-B-Linien: