stylohyoid syndrome




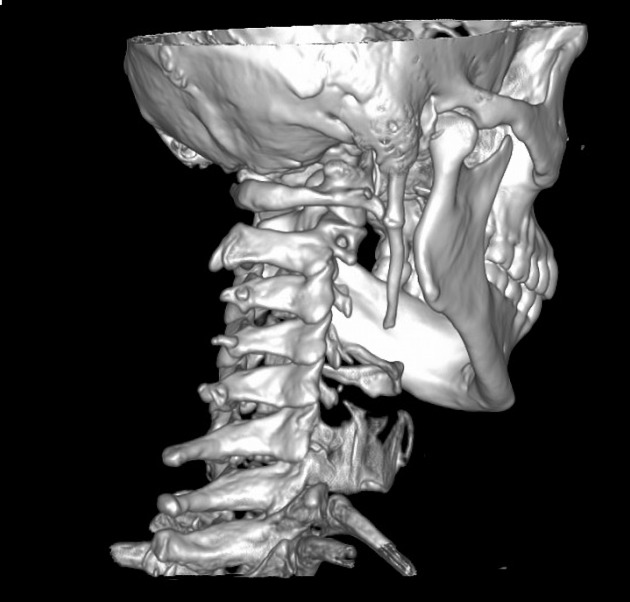






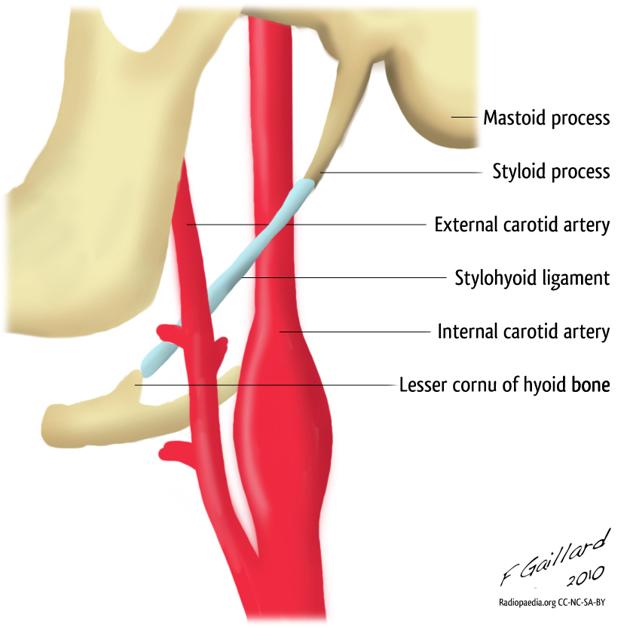









Eagle syndrome refers to symptomatic elongation of the styloid process or calcified stylohyoid ligament . It is often bilateral. In most cases, the cause is unknown; however, the condition is sometimes associated with disorders causing heterotopic calcification such as abnormal calcium/phosphorus metabolism and chronic renal failure.
Clinical presentation
Clinical presentation is varied and establishing a causative relationship between the styloid process/stylohyoid ligament and symptoms can be challenging. Classically, the pain develops following tonsillectomy, presumably due to distortion of the local anatomy following surgery; however, it is frequently found in patients who have not had regional surgery .
The syndrome can be divided into two main subtypes :
- due to compression of cranial nerves
- due to compression of the carotid artery
Cranial nerve impingement
Patients can have symptoms related to compression and irritation of cranial nerves in the region (cranial nerves V, VII, IX and X) such as :
- facial pain when turning the head
- dysphagia
- foreign body sensation
- pain on extending tongue
- change in voice
- sensation of hypersalivation
- tinnitus or otalgia
On palpation of the styloid process tip, symptoms should ideally be exacerbated.
Arterial impingement
Compression of the carotid artery may produce vascular/ischemic symptoms as well as pain along the artery to the supplied territory (thought to be mediated by the sympathetic plexus), including :
- mechanical compression
- visual symptoms
- syncope
- carotid dissection has also been described
- sympathetic plexus irritation (carotidynia)
- eye pain
- parietal pain
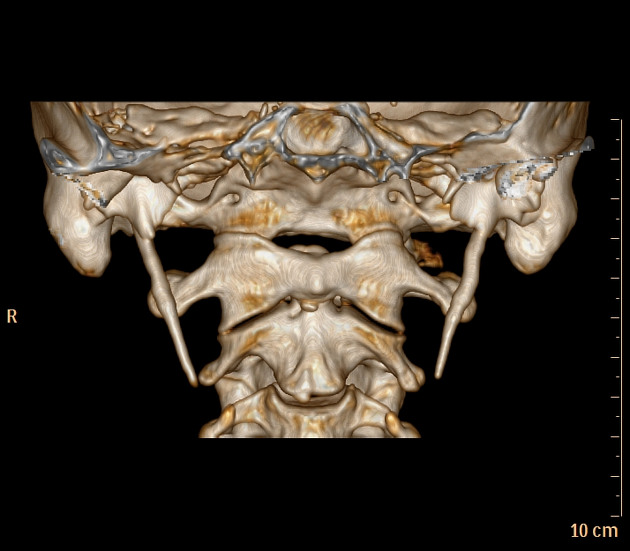
Radiographic features
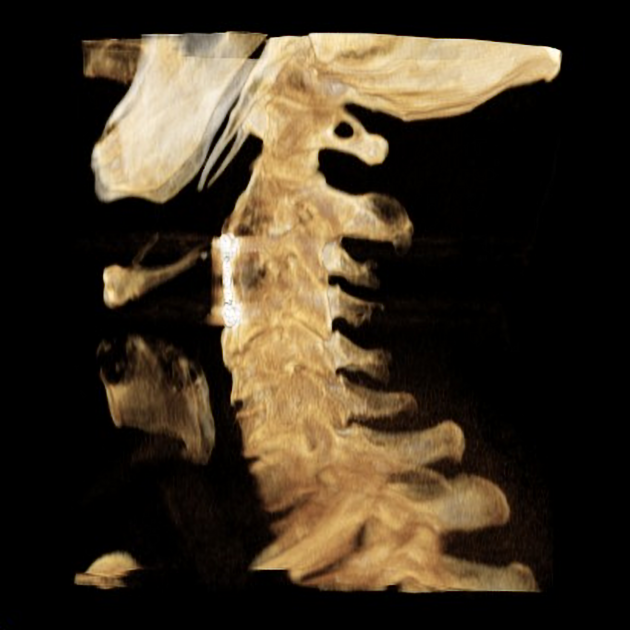
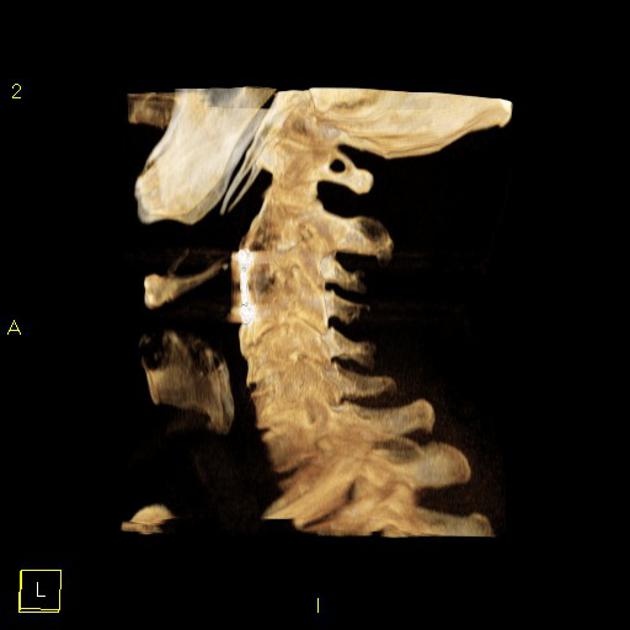
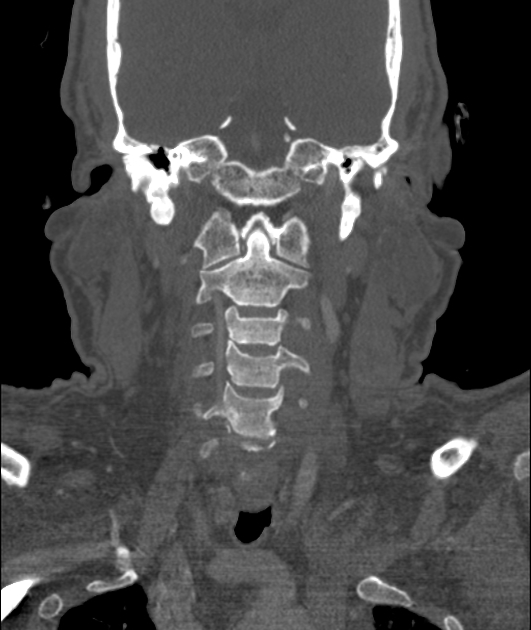
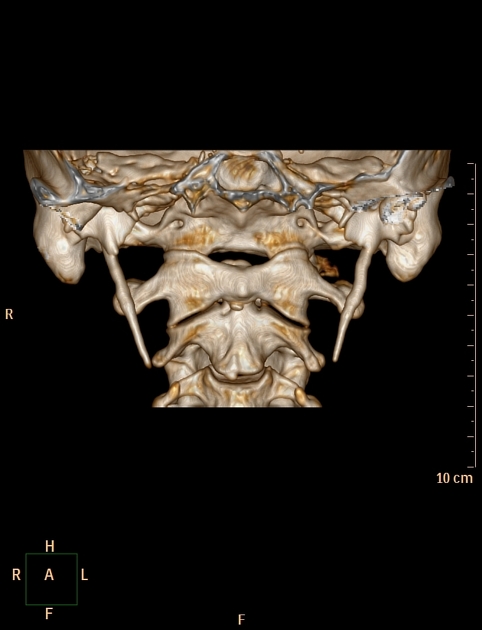
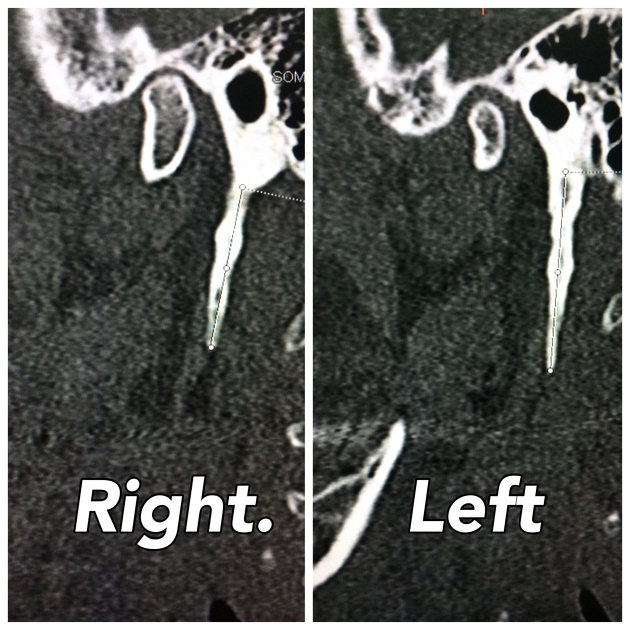
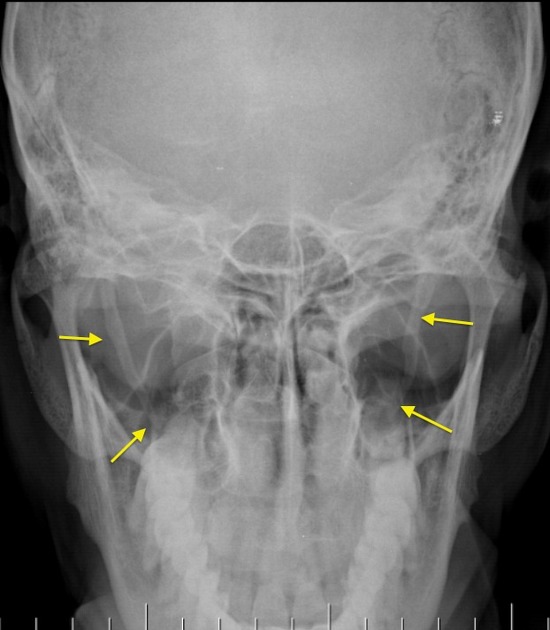
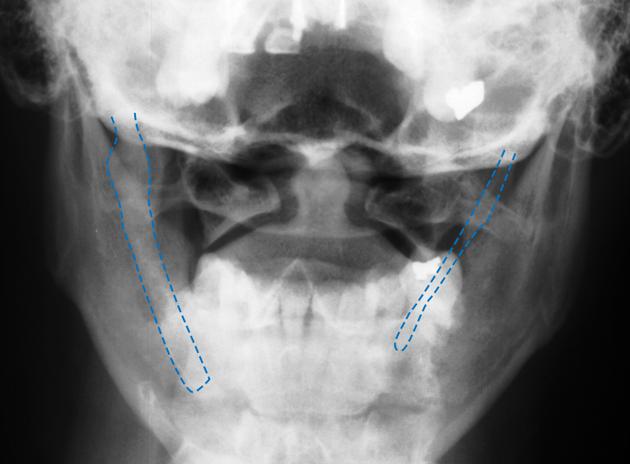
The normal length of the styloid in an adult is thought to be approximately 2.5 cm while an elongated styloid is considered longer than 3 cm. If this definition is used, ~4% of the population have an elongated process; however, only a small proportion of them (4-10%) are symptomatic. Elongation can be unilateral or bilateral .
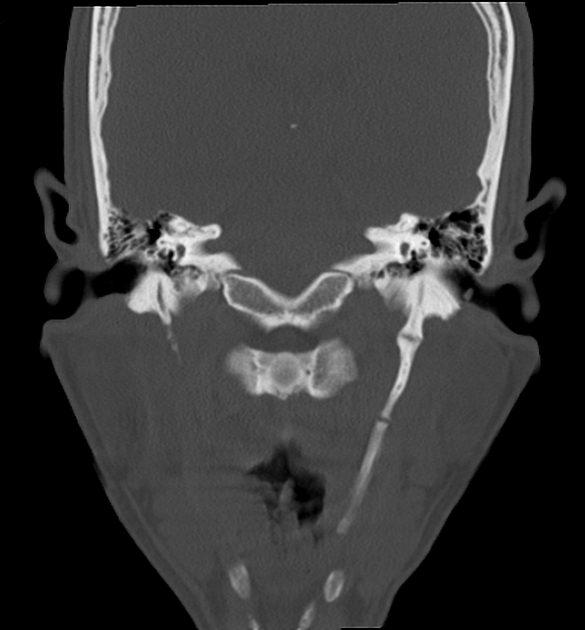
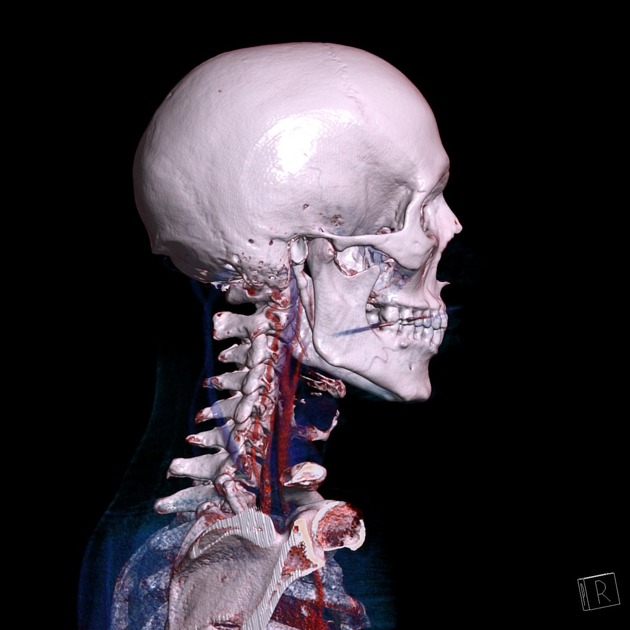
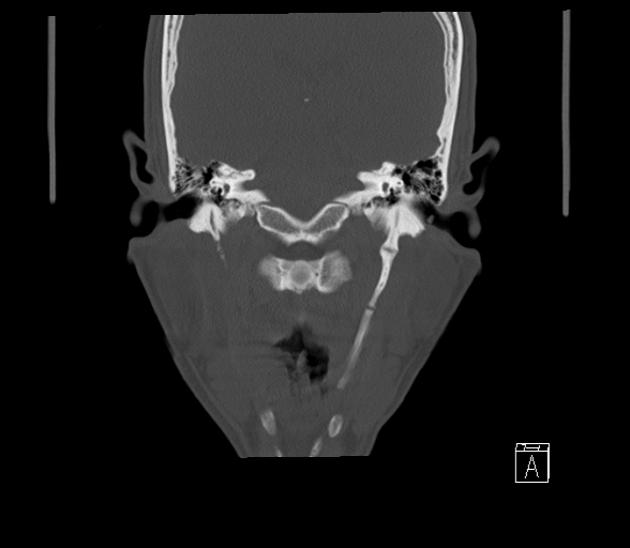
Orthopantomograms and CT can both be used to assess the styloid process/stylohyoid ligament complex.
It has also been proposed that in cases where mechanical vascular compression is the potential cause of ischemic symptoms, an angiographic examination (CT angiography or catheter angiography) obtained with the patient's head positioned to reproduce symptoms may demonstrate mechanical stenosis of the carotid artery .
Treatment and prognosis
In many cases, once the cause of pain has been attributed to the styloid process rather than a more sinister entity, no further treatment is required, or perhaps analgesics can be offered for pain alleviation.
Transpharyngeal injection of steroids/local anesthetic agents has also been attempted .
In severe cases, surgical excision may be performed, either via a transoral approach or a lateral approach. The transoral approach has the disadvantage of increased infection rates, but does not cause external scarring . Pain may persist even after surgical excision in as many as 20% of patients .
History and etymology
It was first described by American otorhinolaryngologist, Watt Weems Eagle (1898–1980), working at Duke University, in 1937 , however, there are reports that ossification of the stylohyoid ligament had been described as early as the 17 century by Italian anatomist at the University of Padua, Pietro Marchetti (1589–1673) .
See also
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Eagle-Syndrom:
Assoziationen und Differentialdiagnosen zu Eagle-Syndrom: 