subchondrale Insuffizienzfraktur des Knies













Subchondral insufficiency fracture of the knee (SIF/SIFK) are stress fractures in the femoral condyles or tibial plateau that occur in the absence of acute trauma, typically affecting older adults.
Terminology
The entity subsumes that previously known as spontaneous osteonecrosis of the knee (SONK/SPONK) or Ahlbäck disease. Recognizing that spontaneous osteonecrosis of the knee was a misnomer and actually represents a subchondral insufficiency fracture that progressed to subchondral collapse with secondary osteonecrosis, the Society of Skeletal Radiology Subchondral Bone Nomenclature Committee recommended that "subchondral insufficiency fracture" be the preferred term .
Epidemiology
Subchondral insufficiency fracture of the knee is seen more frequently in women (M:F 1:3) and affects older patients, typically over the age of 55.
Clinical presentation
Patients often recall an acute onset of severe pain without significant trauma.
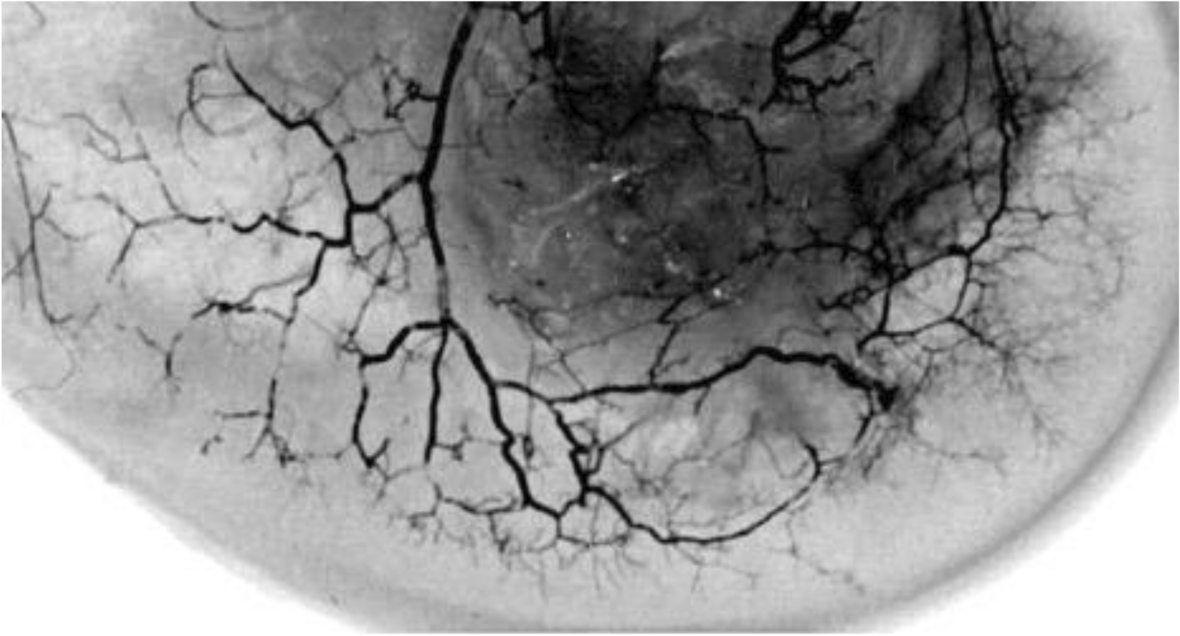
Pathology
By definition, secondary osteonecrosis of the knee occurs secondary to an insult. Subchondral insufficiency fracture of the knee is not thought to be caused by bone death but instead by osteoporosis and insufficiency fractures, with histopathologically proven origins in weakened trabeculae and applied microtraumatic forces .
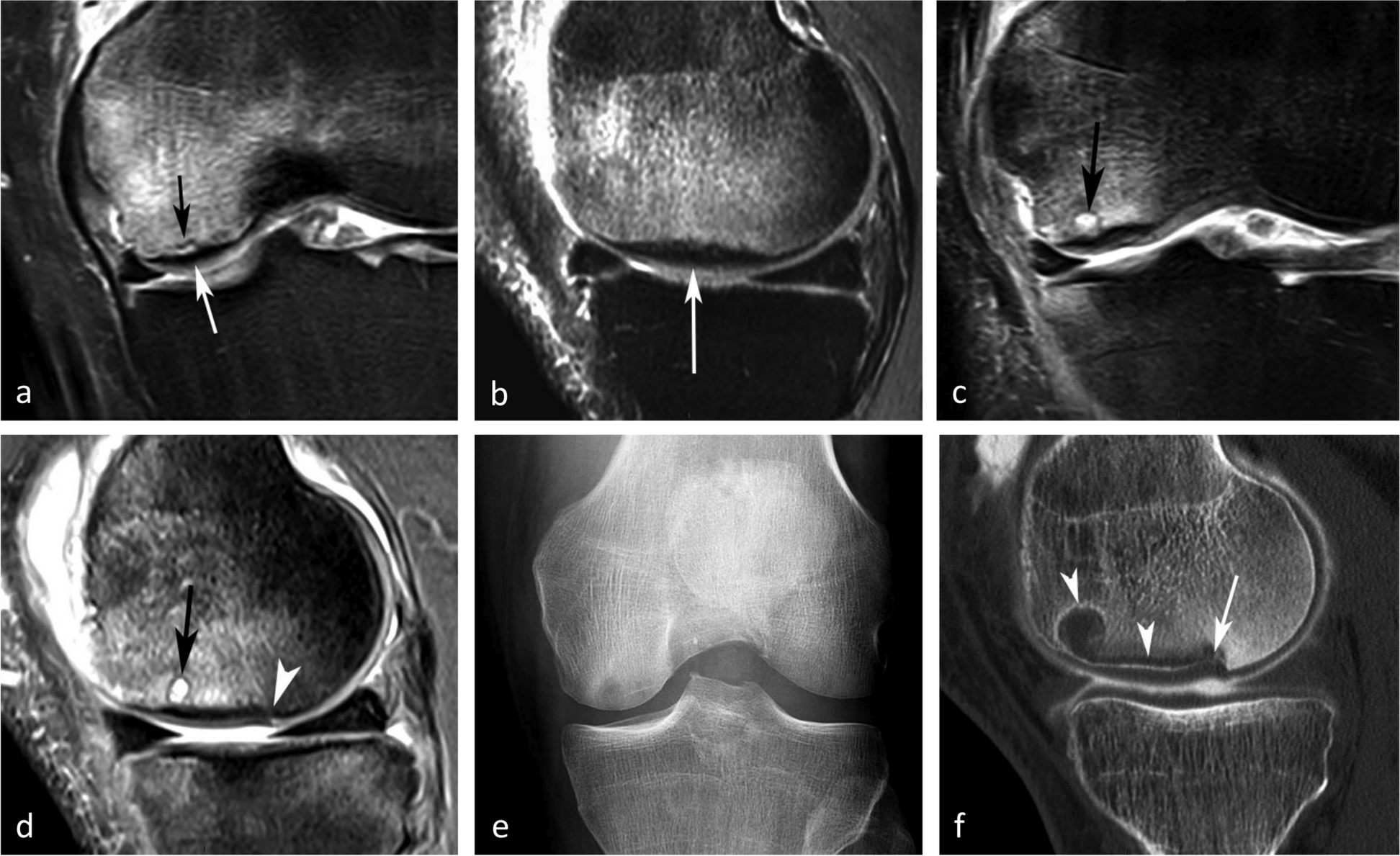
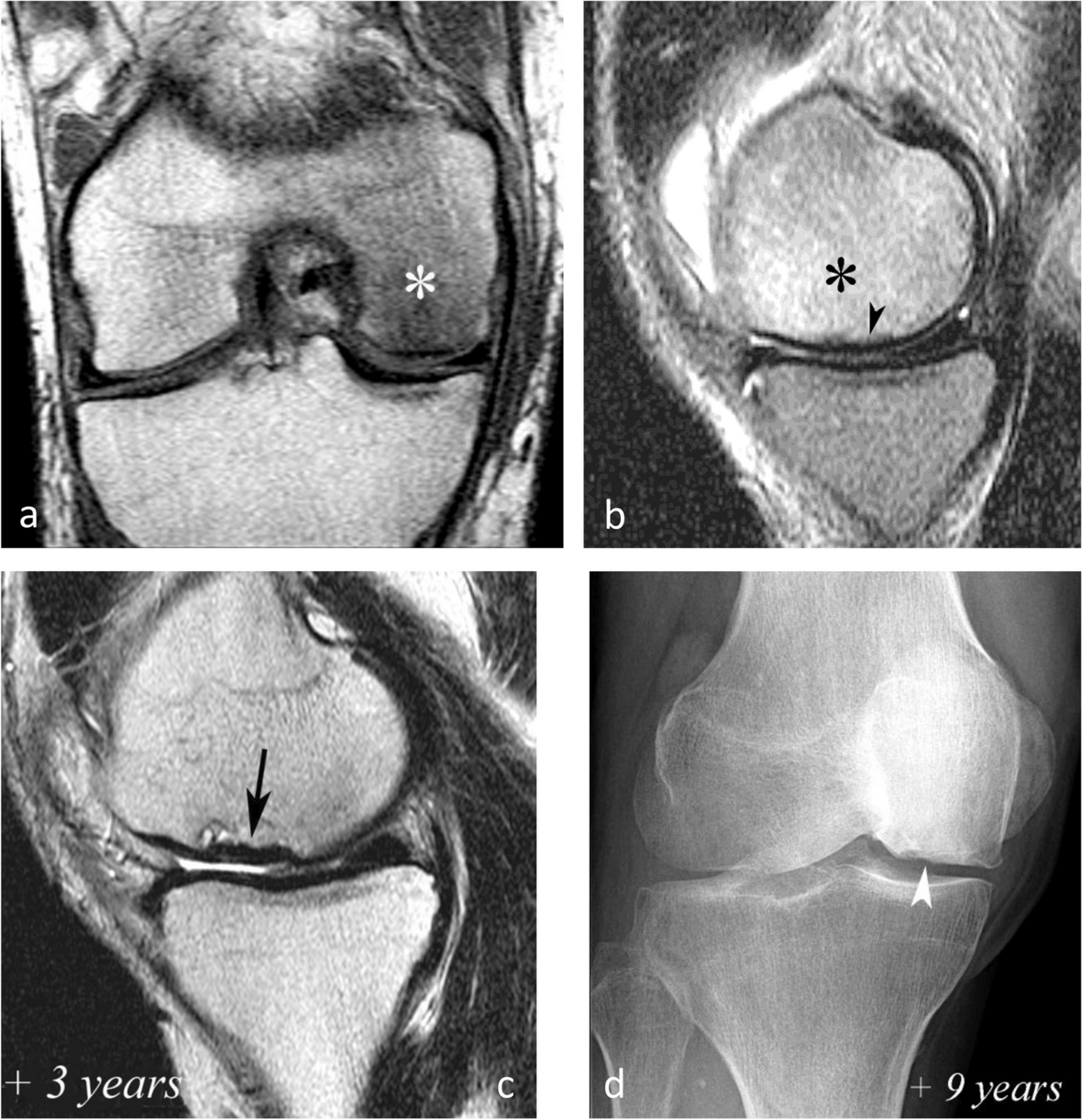
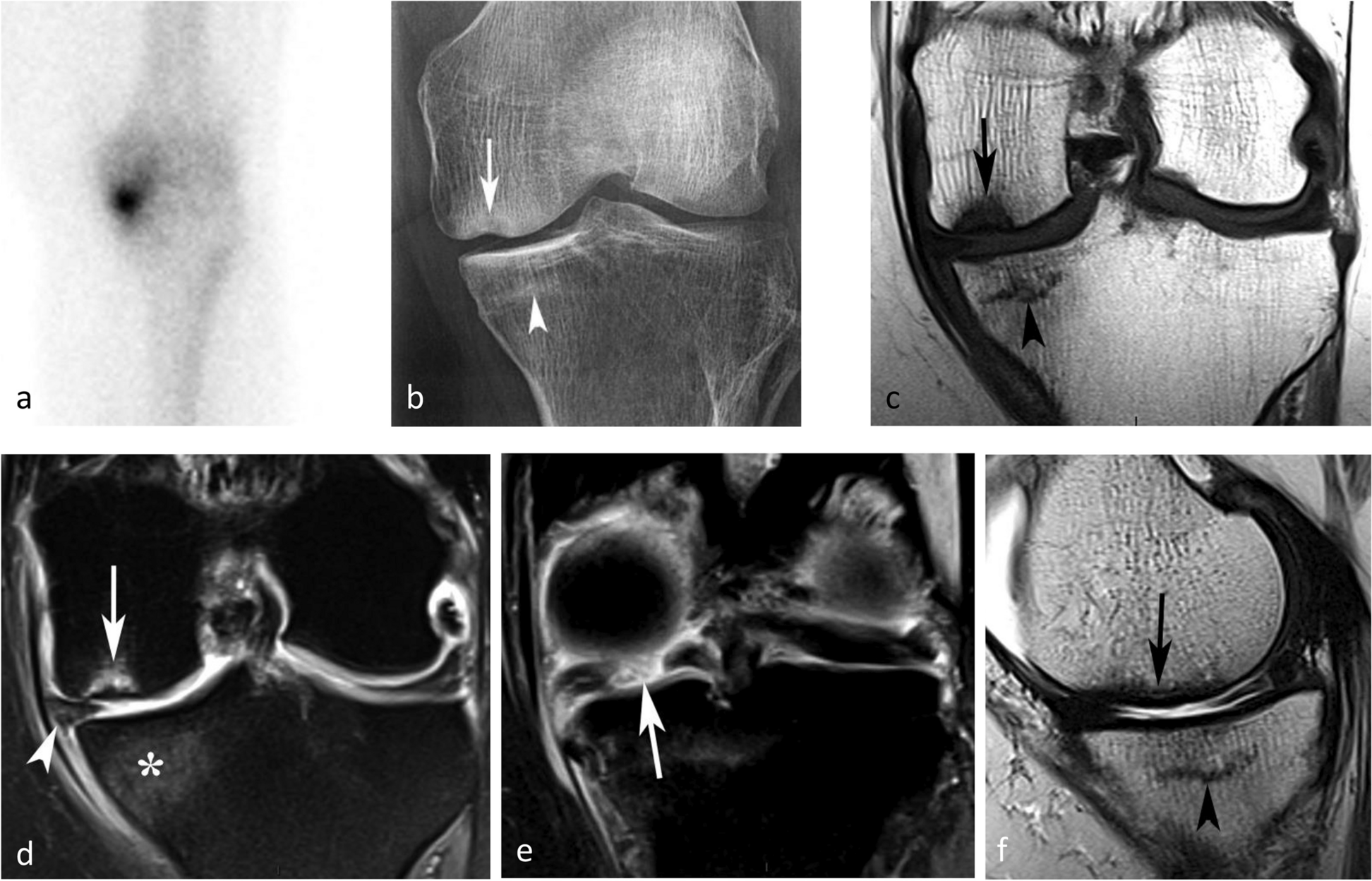
Radiographic features
It is almost always unilateral, usually affects the medial femoral condyle (but can occasionally involve the tibial plateau ) and is often associated with a meniscal tear.
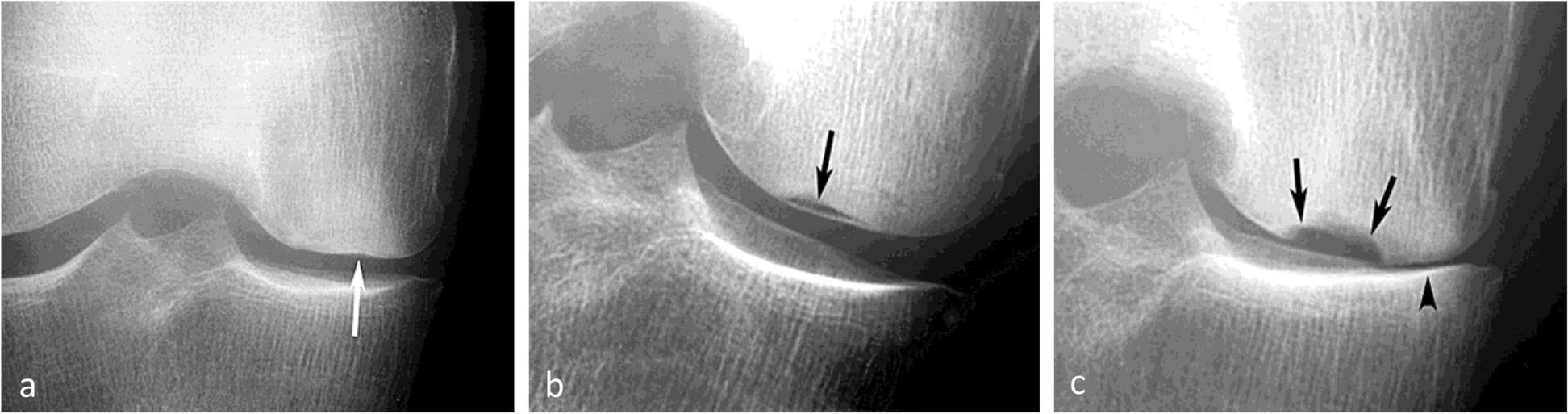
Plain radiograph
In the later stages features seen include:
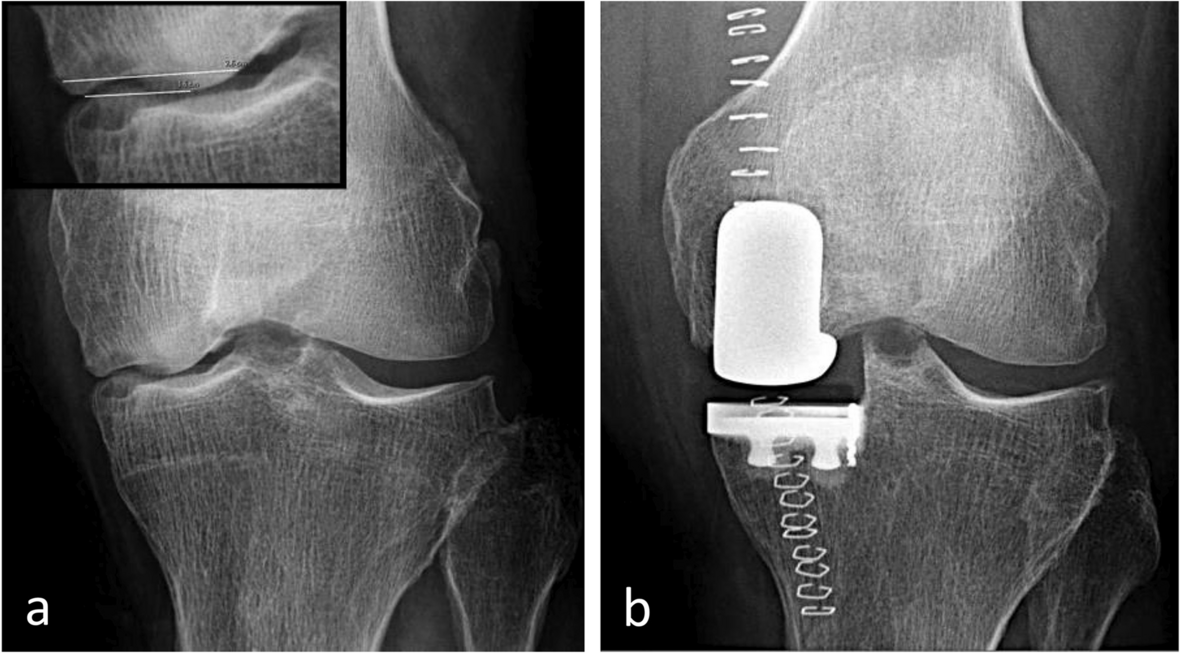
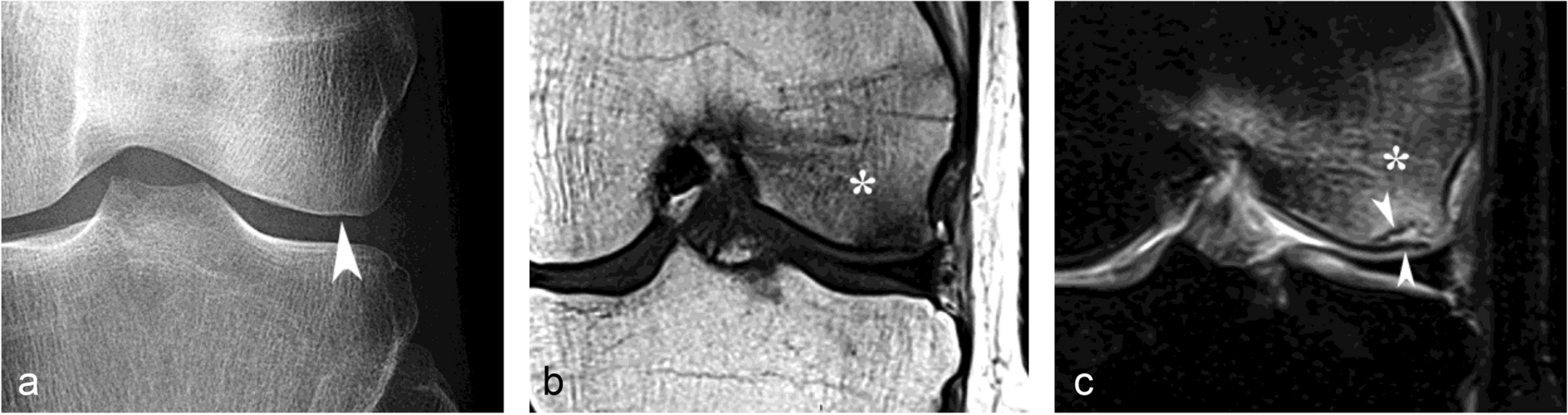
- flattening of the medial femoral condyle
- subchondral radiolucent focus
- complicating subchondral fracture with periosteal reaction
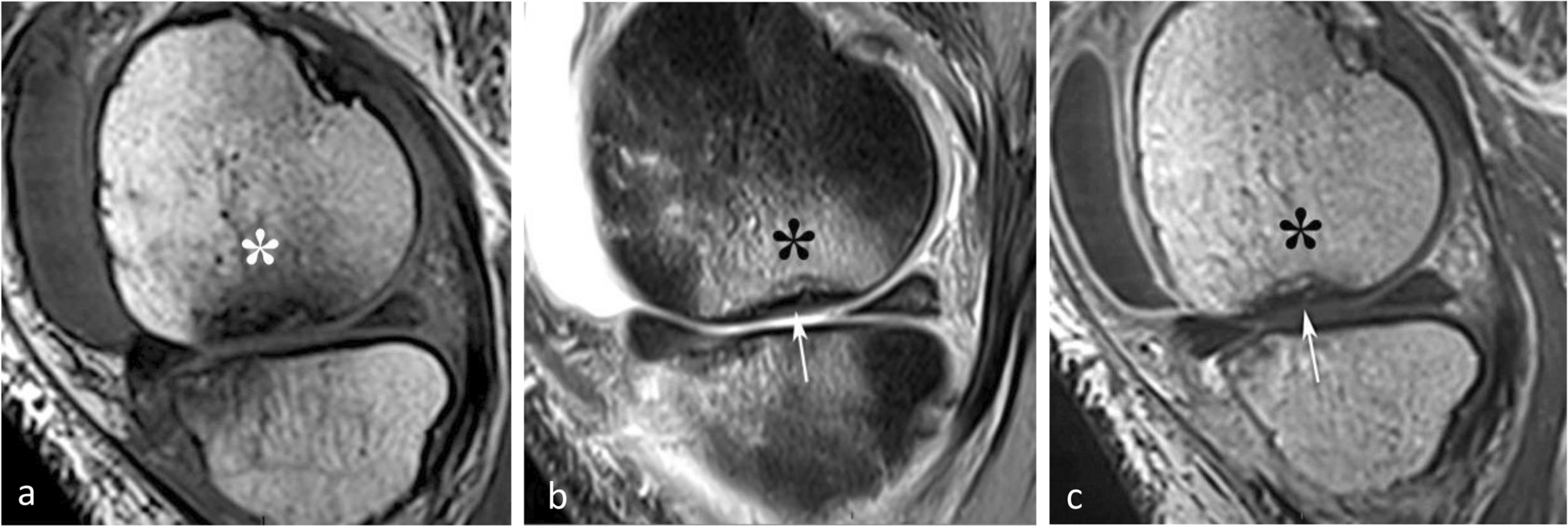
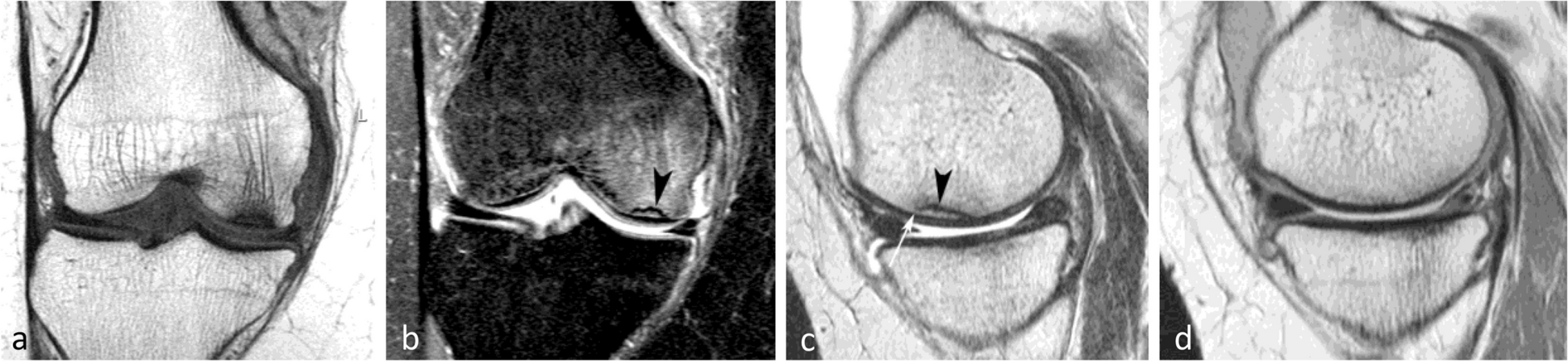
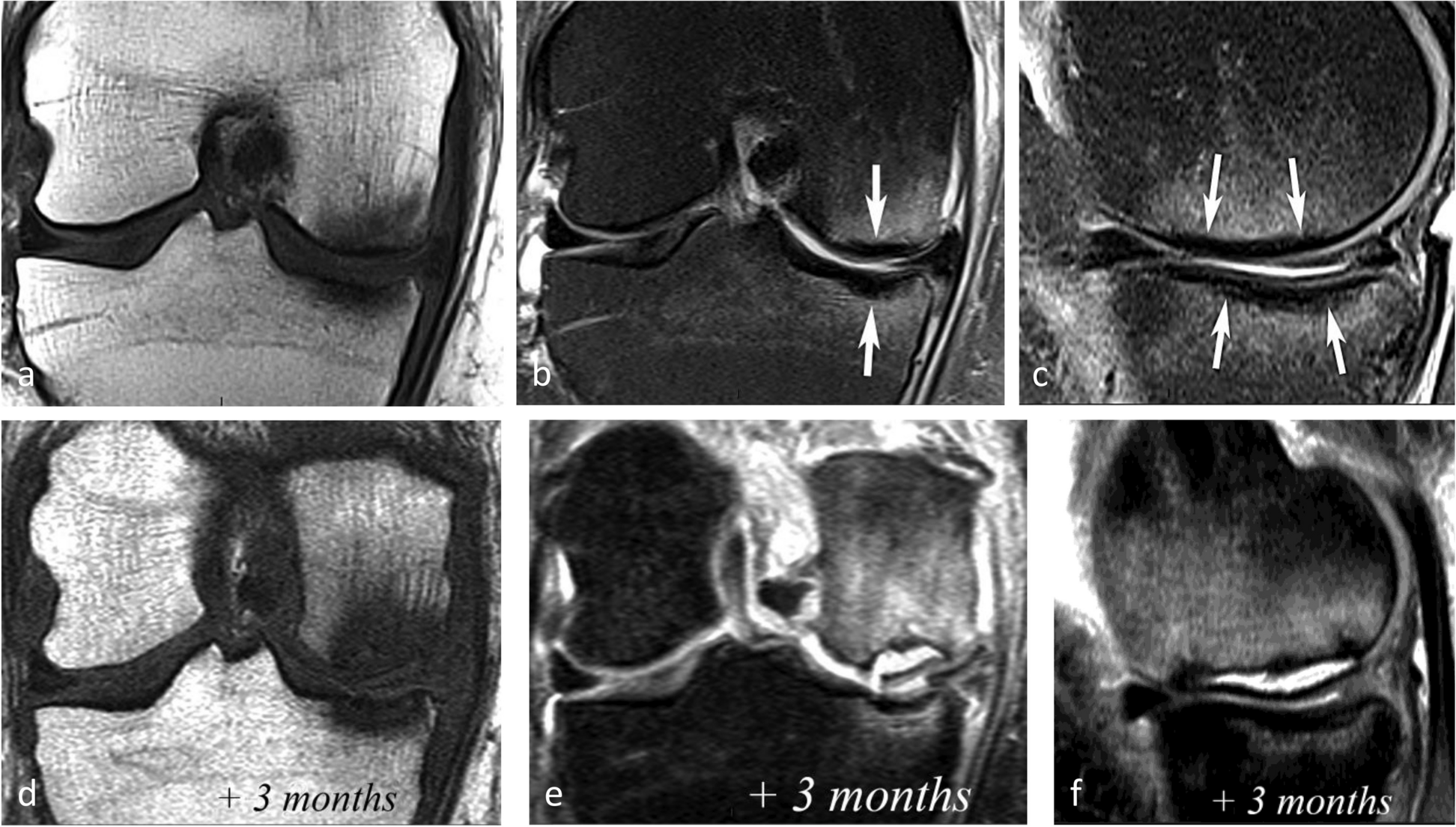
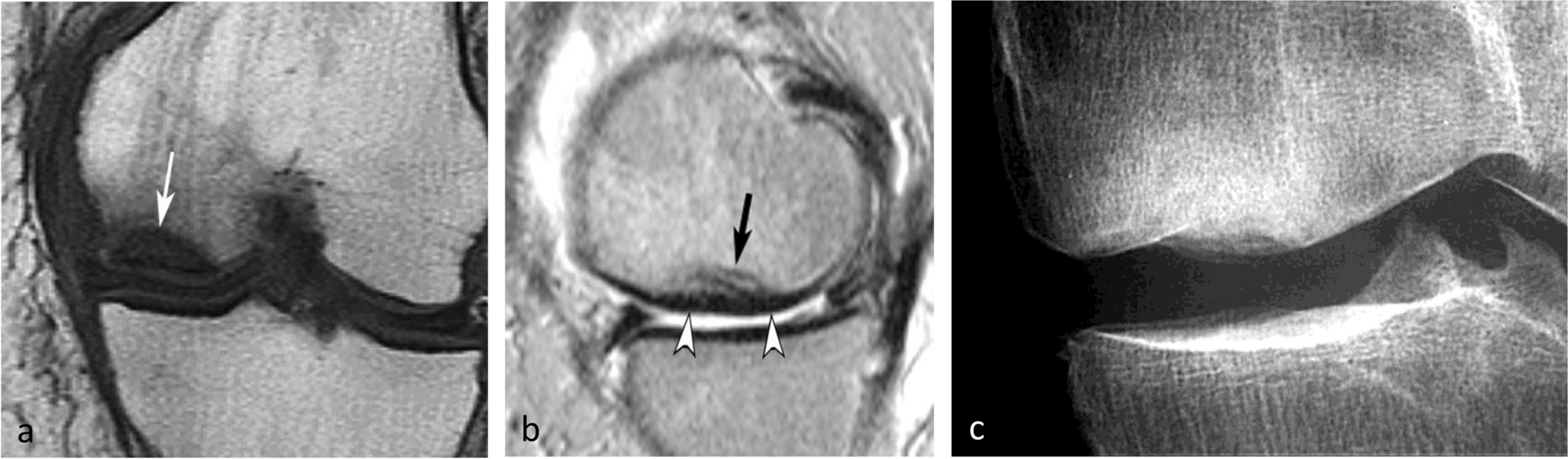
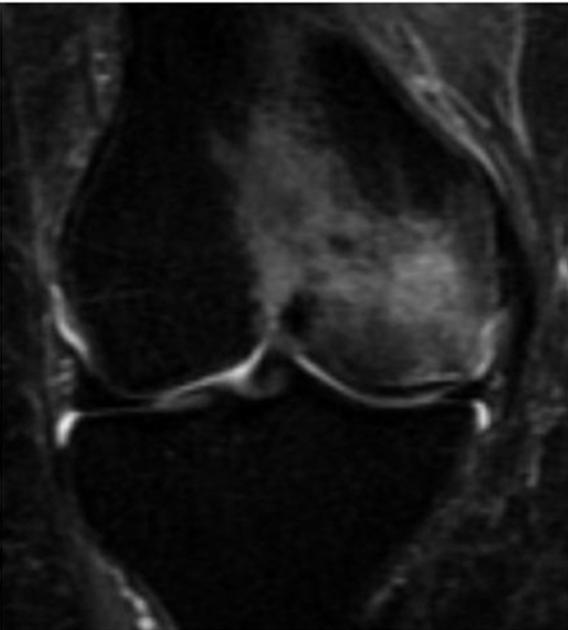
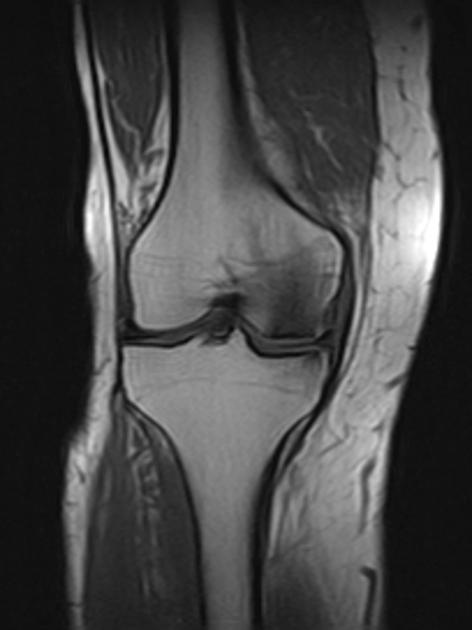
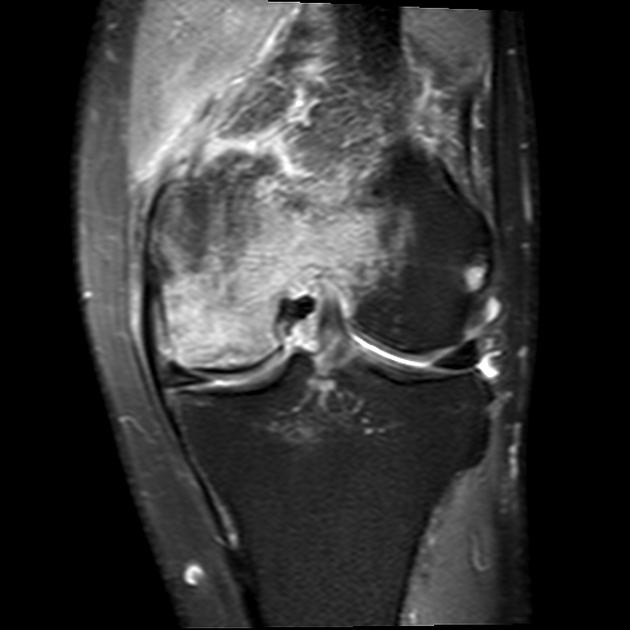
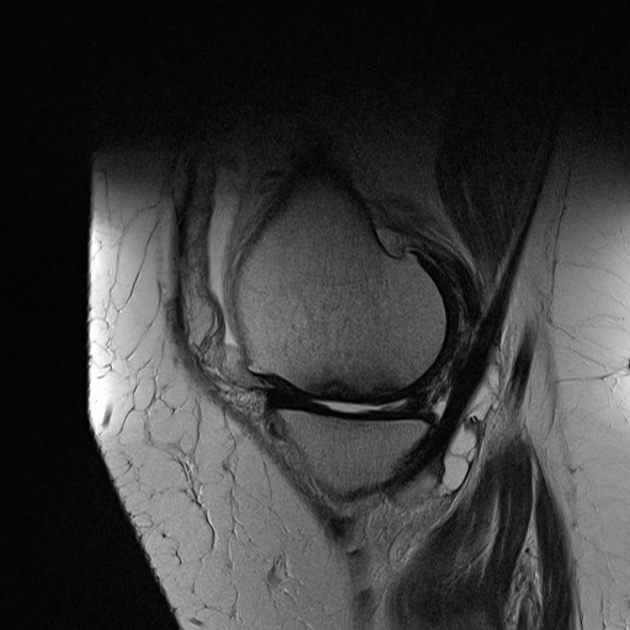
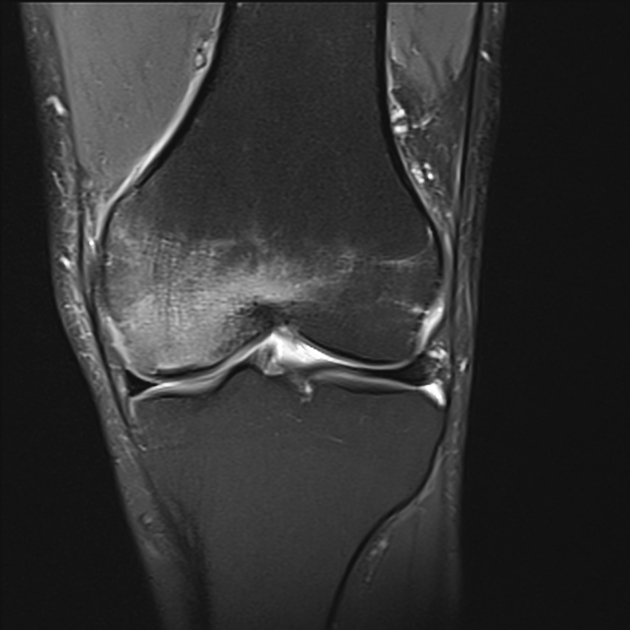
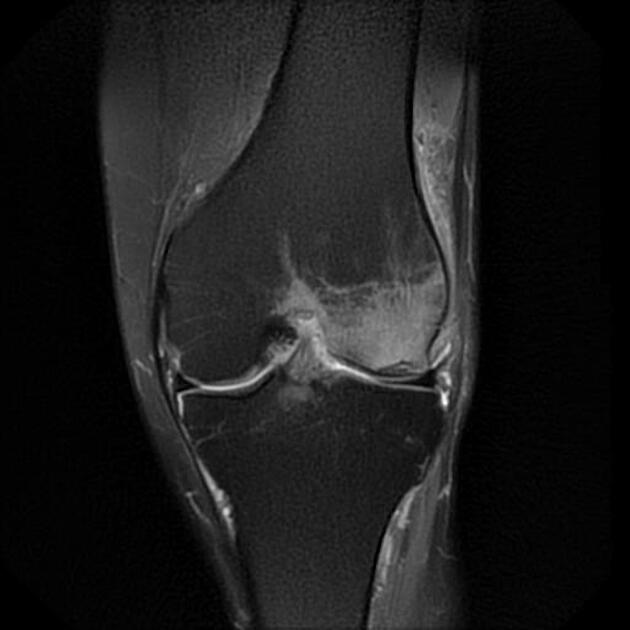
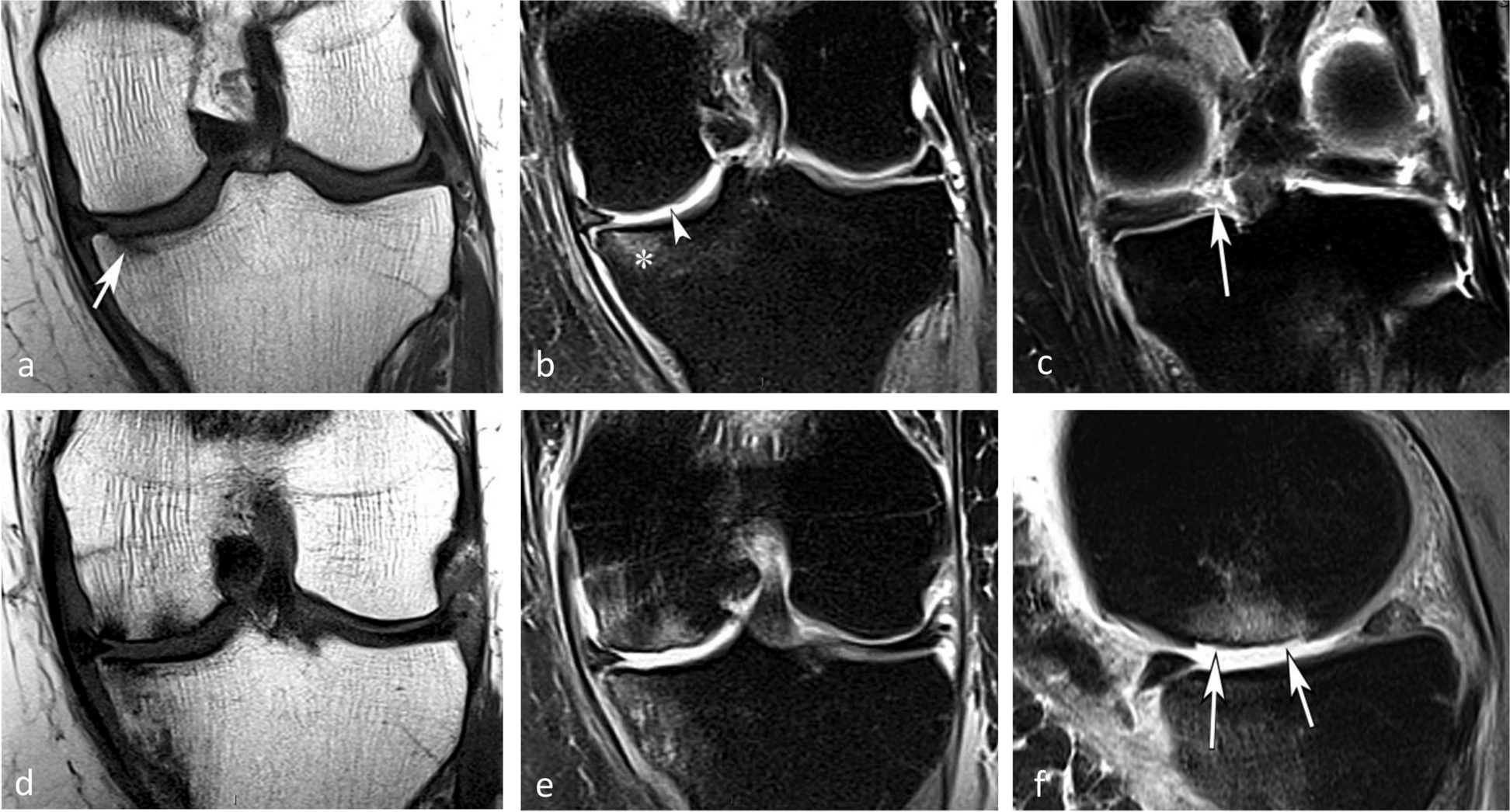
MRI
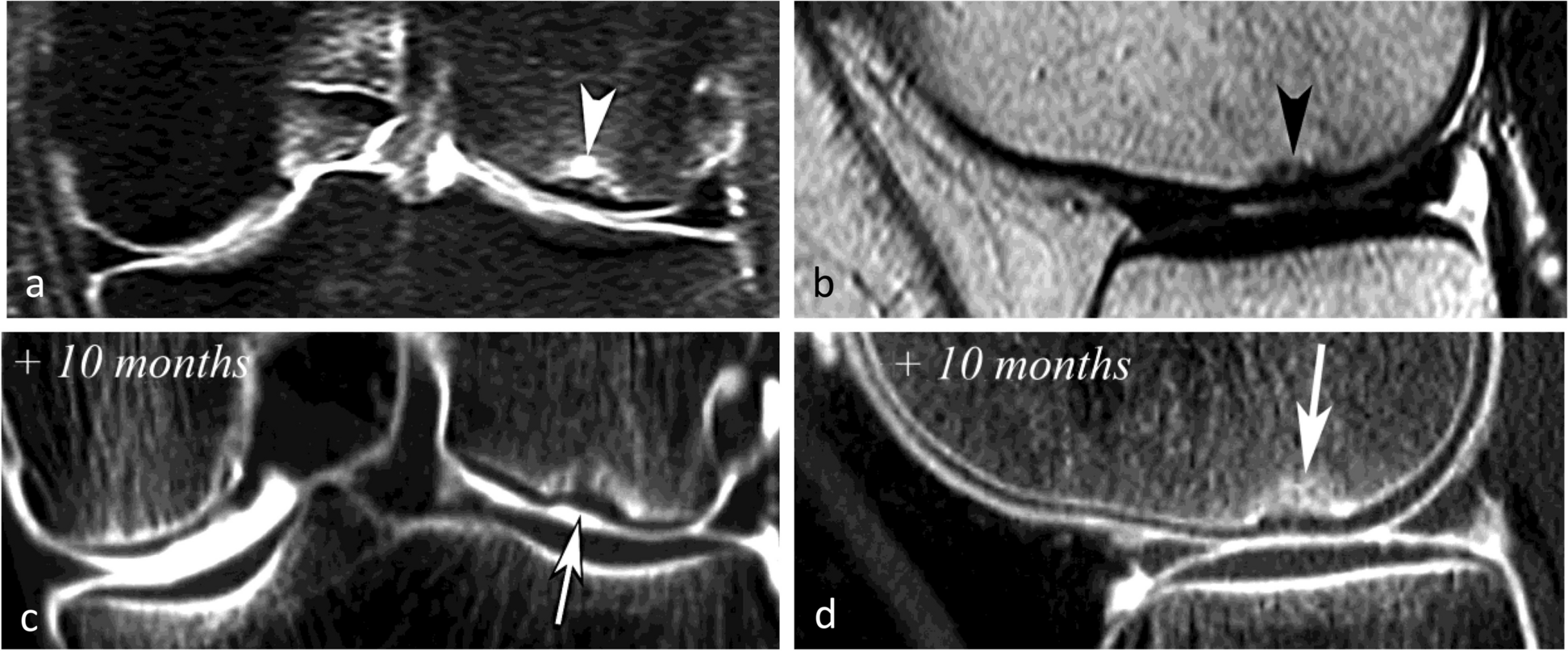
Features can vary depending on the stage and are best characterized on T2-weighted and proton density-weighted sequences. The following criteria apply to lesions without overlying cartilage abnormalities:
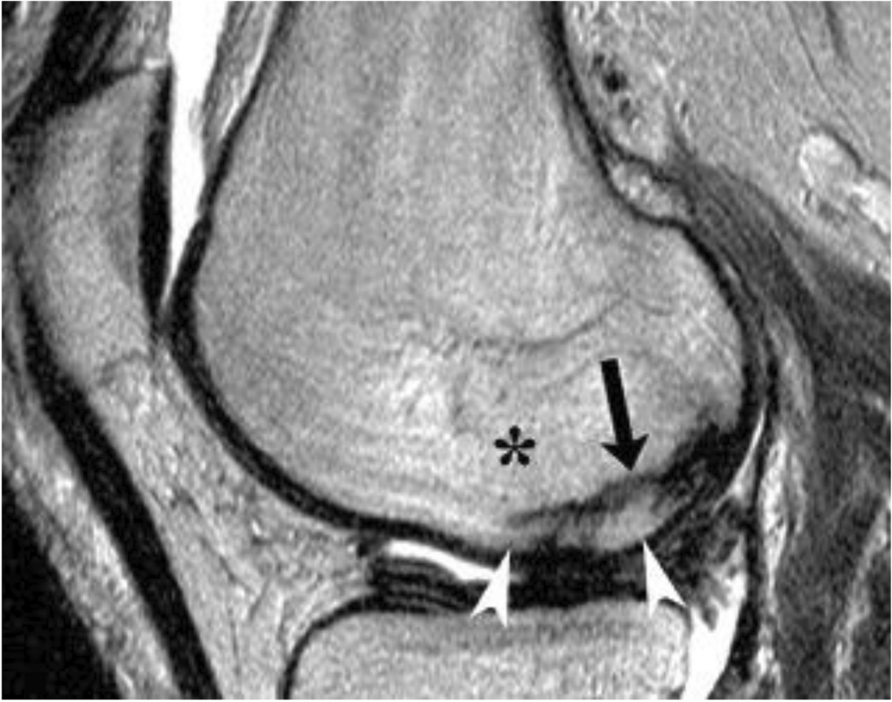
- subchondral bone plate fracture
- in the weight-bearing area of the involved condyle
- subtle flattening or a focal depressive deformity
- an irregular, discontinuous hypointense line in the subarticular marrow, representing callus and granulation tissue
- there may be a fluid-filled cleft within the subchondral bone plate (poor prognostic factor)
- excavated defect of the articular surface (advanced cases)
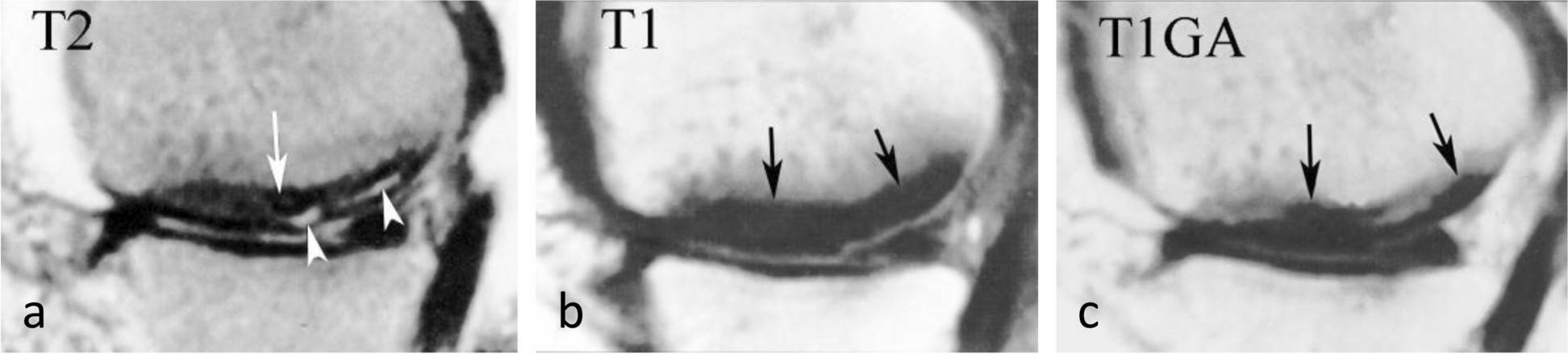
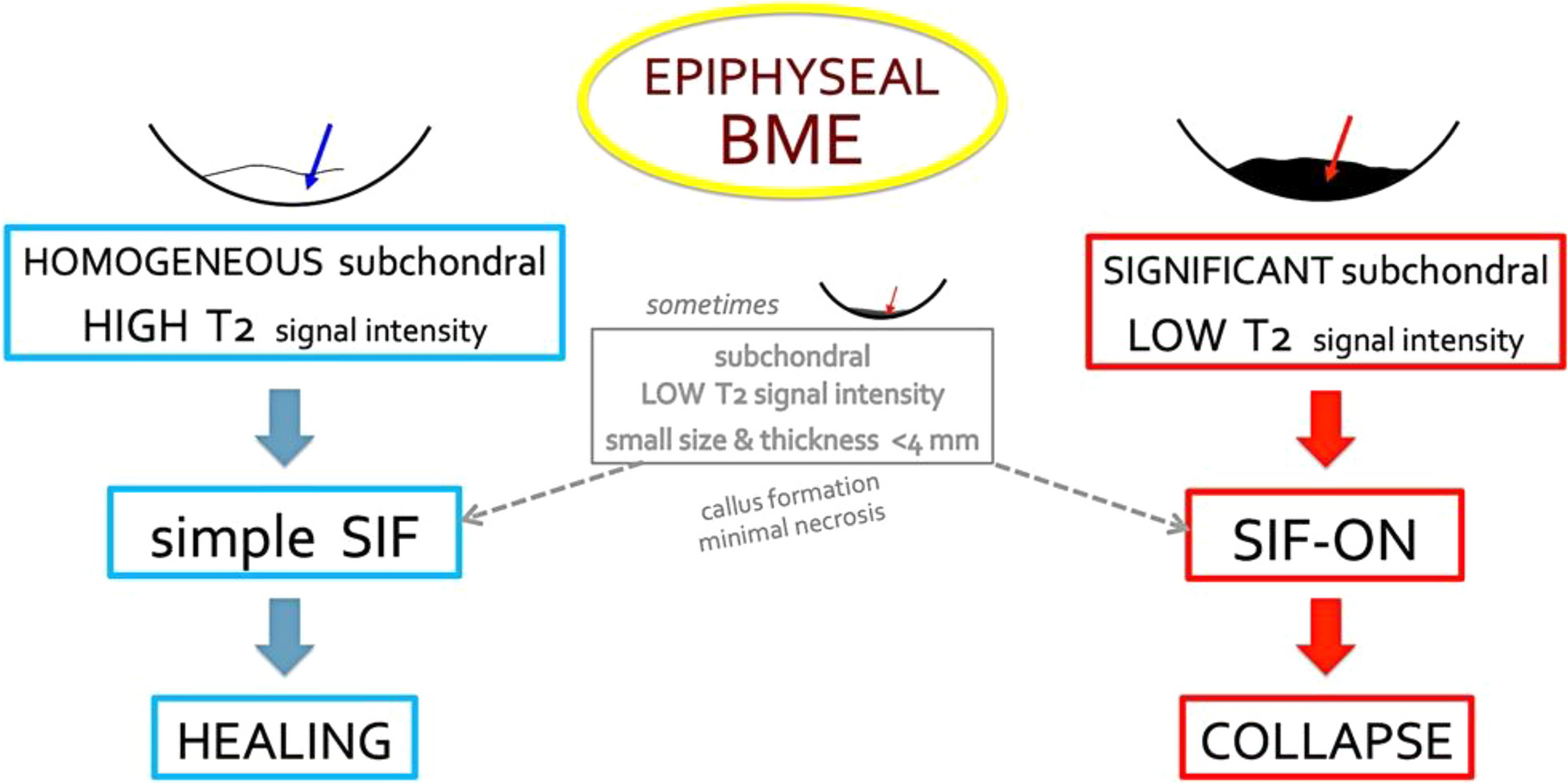
- focal subchondral area of low signal intensity subjacent to the subchondral bone plate representing local ischemia (considered most important in early lesions and a specific MRI finding)
- this area shows no enhancement on post-contrast; if it is thicker than 4 mm or longer than 14 mm, the lesion may be irreversible and may evolve into irreparable epiphyseal collapse and articular destruction
- appears as a thickened subchondral bone plate, which represents a fracture with callus and granulation tissue and secondary osteonecrosis in the subarticular region
- ill-defined bone marrow edema and a lack of peripheral low signal intensity rim as seen in osteonecrosis and bone infarcts
Associated features that may predict prognosis include:
- associated meniscal tear and degree of extrusion
- chondrosis severity
Treatment and prognosis
Prognosis varies from complete recovery to total joint collapse . Treatment can either be operative or non-operative, with initial treatment often conservative and consisting of analgesia and protected weight bearing. Subchondral hypointense fracture lines tend to resolve with conservative therapy. In more advanced cases, subchondroplasty (where a bone substitute is injected) may be considered.
Differential diagnosis
Possible considerations include:
- osteochondritis dissecans of the knee
- subchondral stress/fatigue fracture: overuse injuries in patients without associated risk factors
History and etymology
It was first systematically described by Ahlbäck in 1968 .
Siehe auch:
- Aseptische Knochennekrose
- Morbus Sudeck
- Insuffizienzfraktur
- Osteochondrosis dissecans des Kniegelenks
- Knochenmarködem-Syndrom des Knies
und weiter:


 Assoziationen und Differentialdiagnosen zu subchondrale Insuffizienzfraktur des Knies:
Assoziationen und Differentialdiagnosen zu subchondrale Insuffizienzfraktur des Knies: