wandering spleen










Wandering spleen is a rare condition in which the spleen migrates from its usual anatomical position, commonly to the lower abdomen or pelvis.
Epidemiology
Wandering spleen is rare, with a reported incidence of <0.5%.
Diagnosis is most commonly made between ages 20 and 40 years and is more common in multiparous women .
Clinical presentation
Wandering spleen can be an elusive diagnosis as its presentation is greatly variable and intermittent torsion can cause non-specific signs and symptoms.
It can present as an asymptomatic or painful abdominal mass, intermittent abdominal pain, or as an acute abdomen (e.g. bowel obstruction, acute pancreatitis) .
Pathology
The abnormal mobility of the spleen is caused by an abnormality of its suspensory ligaments. There may be a congenital absence or underdevelopment of these ligaments, or an acquired laxity of the ligaments caused by various conditions, such as pregnancy or diseases causing splenomegaly. Due to these abnormal ligaments a long vascular pedicle may form, containing the splenic vessels, predisposing the spleen to torsion and consequently splenic infarction .
Etiology
There are various causes, mostly related to the splenomegaly.
Radiographic features
The often non-specific clinical presentation of wandering spleen makes radiological evaluation invaluable in its diagnosis. Performing the radiological investigations in different positions allows identification of the wandering spleen’s inclination to wander.
Plain radiograph
A wandering spleen is not frequently diagnosed on plain film radiography, but findings on abdominal x-ray may include :
- absence of splenic shadow in the left upper quadrant
- space-occupying soft tissue mass in abnormal location
- distended bowel loops
Ultrasound
Can be used to identify an abnormal anatomical position of the spleen, usually low-lying, or an absence of the spleen in the left upper quadrant . It has been described that the mobility of the spleen can be demonstrated when scanning in the right decubitus position, with migration of the spleen to the dependent position on the right side . There may also be a finding of a characteristic comma-shaped spleen in an extra-anatomical position .
Doppler ultrasound
Doppler ultrasound can demonstrate the vascular flow to the spleen and help diagnose splenic torsion or infarction .
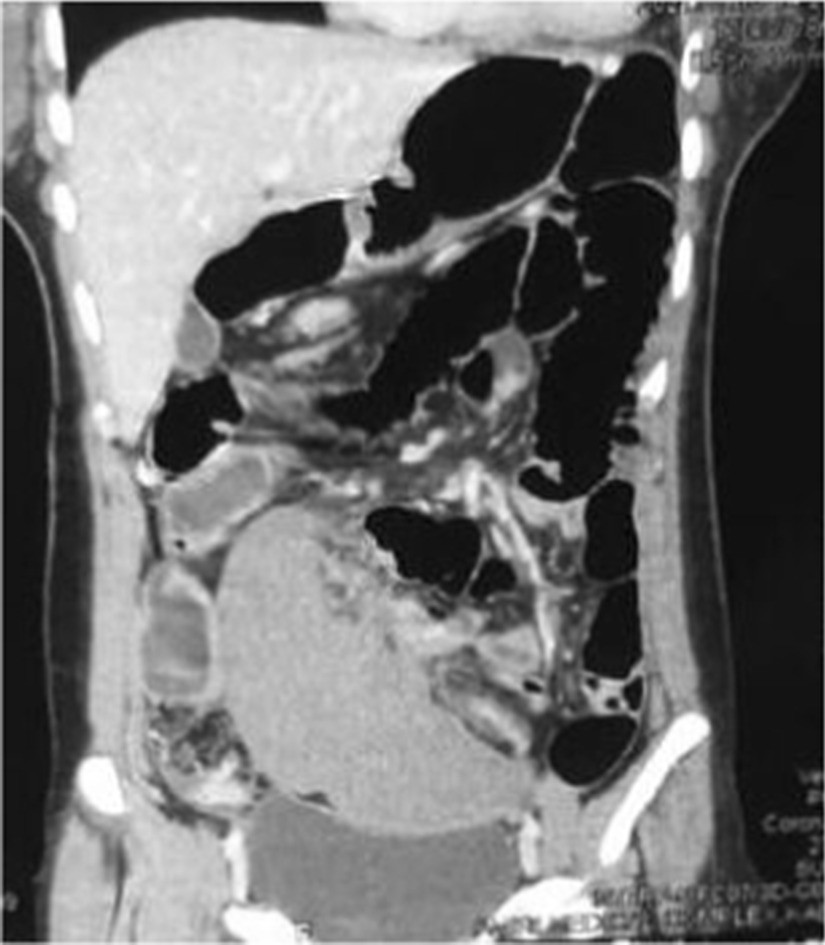
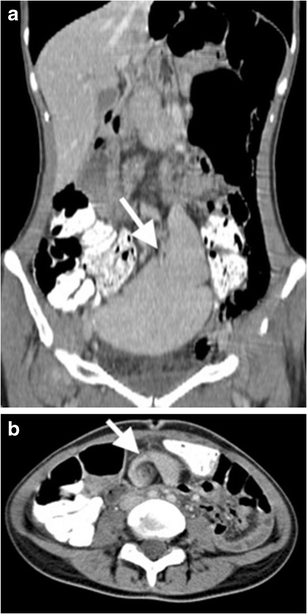
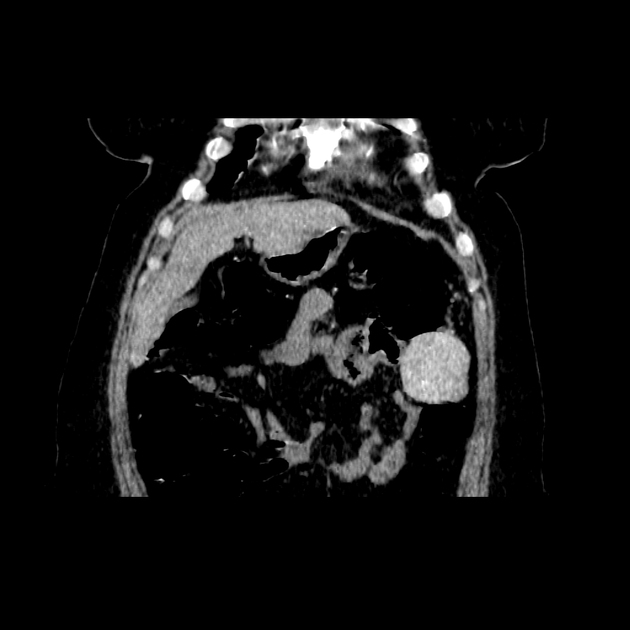
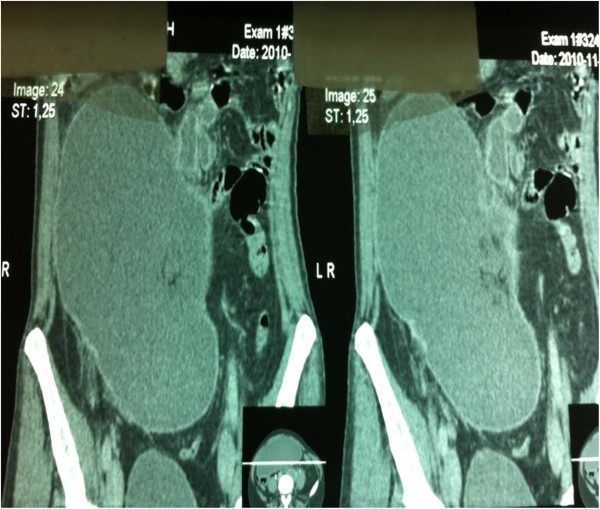
CT
CT with contrast can be useful in identifying the displaced spleen and demonstrating the degree of organ ischemia in the setting of torsion and infarction of the spleen .
Possible findings include :
- absence of the spleen in the left upper quadrant
- ovoid or comma-shaped abdominal mass
- whirl sign: whirled appearance of hyperdense, non-enhancing splenic vessels
- enlarged spleen, with minimal or no enhancement
- signs of splenic hypoperfusion: heterogeneous, capsular (rim-like) or globally decreased enhancement
Nuclear medicine
Technetium sulfur colloid liver-spleen scan can be used to identify an abnormal abdominal mass as the spleen .
Treatment and prognosis
Wandering spleen is treated surgically, ideally by detorsion and splenopexy. However, if there is evidence of hypersplenism, thrombosis, or infarction, splenectomy may be necessary. Laparoscopic techniques for both splenopexy and splenectomy are preferred, as they offer the benefits of minimally invasive surgery .
Siehe auch:
- mechanischer Ileus
- Nebenmilz
- Splenose
- Akute Pankreatitis
- pseudocyst
- splenosis consecutive to trauma
- Milztorsion
- ektopes Lebergewebe
und weiter:


 Assoziationen und Differentialdiagnosen zu ektopes Milzgewebe:
Assoziationen und Differentialdiagnosen zu ektopes Milzgewebe:



