intradurales spinales Lipom
Intradural lipomas are a subset of spinal lipomas. They are typically intradural, subpial, juxtamedullary lesions although they have occasionally been reported as entirely intramedullary lesions .
Mature fatty tissue within the spinal dura can be seen in a number of entities:
- lipomyelocele/lipomyelomeningocele: 84%
- lipoma of the filum terminale: 12%
- intradural lipoma: 4%
This article relates specifically to intradural lipomas. Lipomyelocele/lipomyelomeningocele and lipoma of the filum terminale are discussed separately.
Epidemiology
Intradural spinal lipomas typically present around the second and third decades of life. Males and females are equally affected.
Vertebral and dermal abnormalities are not a feature of these lesions as they are with the more commonly seen lipomas associated with forms of dysraphism.
Clinical presentation
Patients present with neurological deficits secondary to mass effect. The most frequently reported clinical presentation is numbness or spastic weakness in the extremities. Back pain may occur. Radicular pain is uncommon .
Pathology
Intradural spinal lipomas consist of normal fat. Although the pathophysiology of these lesions is poorly understood they are not considered neoplastic.
Radiographic features
General
Intradural lipomas may occur anywhere in the spinal canal. In adults, they are most commonly found in the thoracic region, whereas in children the cervical spine appears to be the most common site .
They usually occur along the dorsal midline of the spinal cord. The spinal cord is flattened ventrally.
Plain film
Widening of the spinal canal with spreading and thinning of the pedicles.
CT
The lesion is classically homogeneously of low (fat) attenuation, without solid or enhancing components.
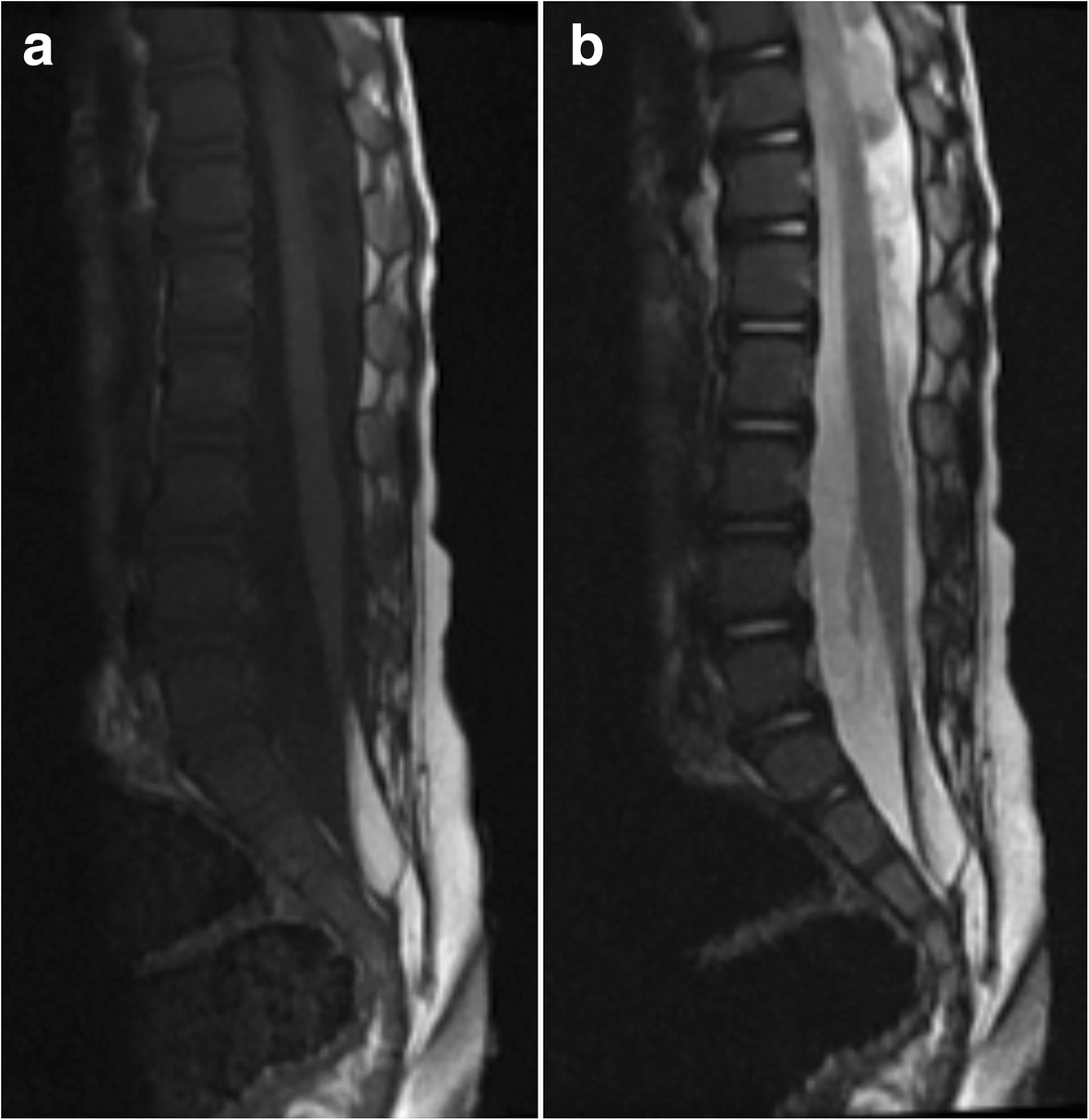
MRI
Intradural spinal lipomas are sharply circumscribed masses largely conforming to the dura but distorting the cord. They follow fat signal on all sequences:
- T1: hyperintense
- T2: hyperintense
- T1 C+ (Gd): no enhancement
- fat-suppressed sequences: hypointense
A chemical shift artefact may be seen.
Treatment and prognosis
The treatment of choice is surgical resection. As lipomas adhere closely to the adjacent spinal parenchyma, they generally cannot be entirely resected and the aim of surgery is decompression .
Because these lesions are typically very slow growing, a very satisfactory and long-lasting clinical effect may be obtained after achieving a subtotal excision .
Differential diagnosis
- lipomyelomeningocele
- is a form of occult spinal dysraphism
- mass is often palpable
- may have cutaneous stigmata
- lipoma of the terminal filum
- fatty infiltration of the filum terminale
- dermoid cyst
- mixed-signal intensity
- may be associated with a dermal sinus
See also
Siehe auch:


 Assoziationen und Differentialdiagnosen zu intradurales spinales Lipom:
Assoziationen und Differentialdiagnosen zu intradurales spinales Lipom: