Para-esophageal hernia







Para-esophageal hernias (POH), or rolling hernias, are an uncommon type of hiatal hernia representing ~10% of all hiatal hernias. The majority of the hiatal hernias being of the sliding type.
Clinical presentation
Can vary and can include:
- asymptomatic
- gastro-esophageal reflux disease (mainly hiatus hernia)
- substernal, post-prandial chest pain
- epigastric pain
- dysphagia
- nausea/vomiting
- obstruction
- diaphragmatic impingement on the stomach
- gastric volvulus
- compression of the esophagus by the intrathoracic stomach
- respiratory complications
- associated with a large para-esophageal hernia
- recurrent aspiration, pneumonia, and chronic cough
Pathology
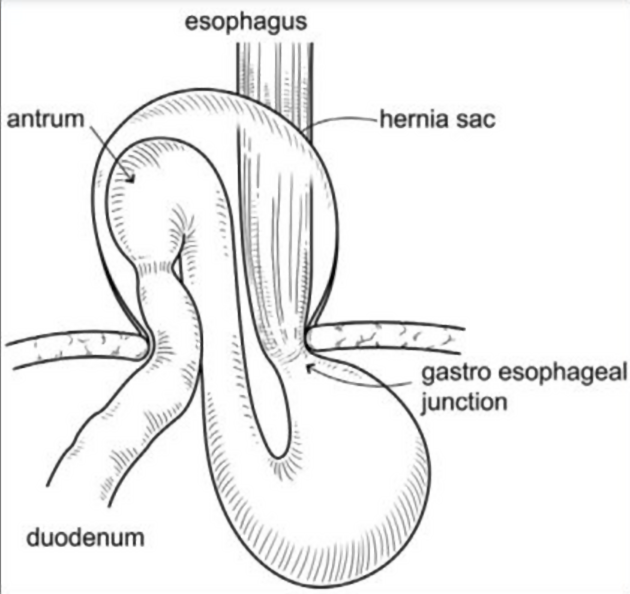
A para-esophageal hernia includes a peritoneal layer that forms a true hernia sac, distinguishing it from the more common sliding hiatal hernia.
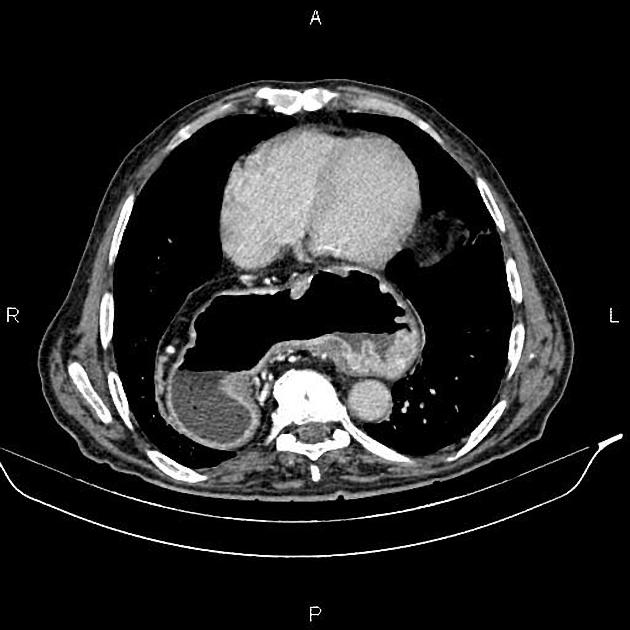
In para-esophageal hernia, there is an upward dislocation of the gastric fundus alongside a normally positioned gastroesophageal junction. The gastric fundus and sometimes abdominal viscera protrude into the mediastinum through the defect in the diaphragm.
In contrast, a sliding hernia does not have a hernia sac and slides into the chest since the gastro-esophageal junction (GEJ) is not fixed inside the abdomen.
Classification
Generally, a hiatus hernia is classified into four types.
- type I - sliding hernia: GEJ migrates into the posterior mediastinum through the esophageal hiatus
- type II-IV - para-esophageal hernias
- type II: occurs when the fundus herniates through the hiatus alongside a normally positioned GEJ
- type III: is a combination of types I and II hernias with a displaced GEJ as well as hernia sac containing portions of the fundus/body of stomach protruding through the hiatus
- type IV: characterized by displacement of the stomach along with other organs (colon, spleen, pancreas and small bowel) into the thorax
Treatment and prognosis
Surgical management is indicated when medical management fails to control symptoms of gastro-esophageal reflux that may be related to the POH, or when there is an emergent complication.
According to the Society of American Gastrointestinal and Endoscopic Surgeons 2013 guidelines:
- in the absence of reflux disease, repair of a type I hernia is unnecessary
- all symptomatic paraesophageal hiatal hernias (types II-IV) should be repaired, especially in the presence of acute obstructive symptoms or volvulus
Differential diagnosis
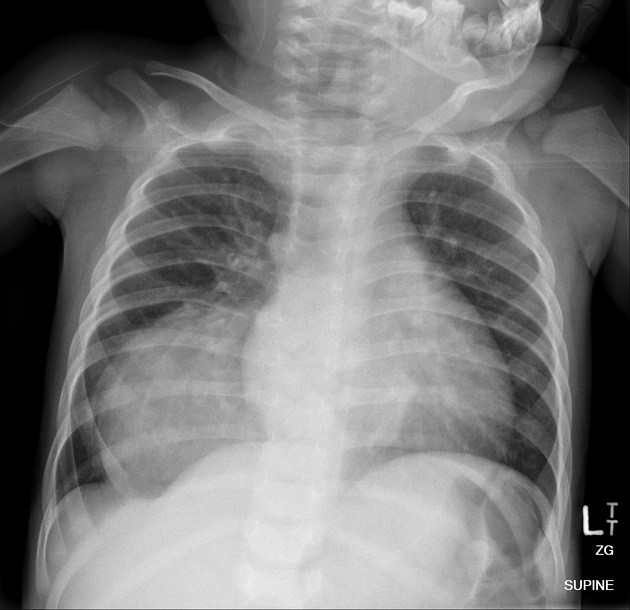
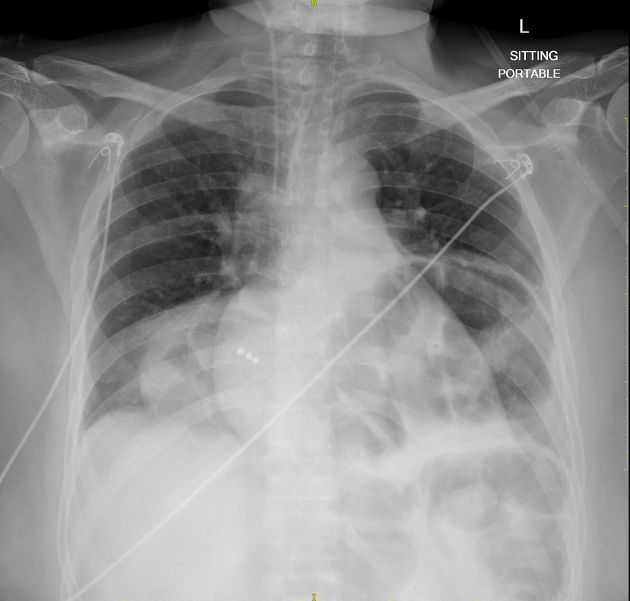
On a chest radiograph, possible considerations include:
- lung abscess
- lower esophageal duplications cyst
- lower thoracic aortic aneurysm
- neurenteric cyst
- epiphrenic diverticulum
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Paraösophageale Hernie:
Assoziationen und Differentialdiagnosen zu Paraösophageale Hernie: