Skoliose


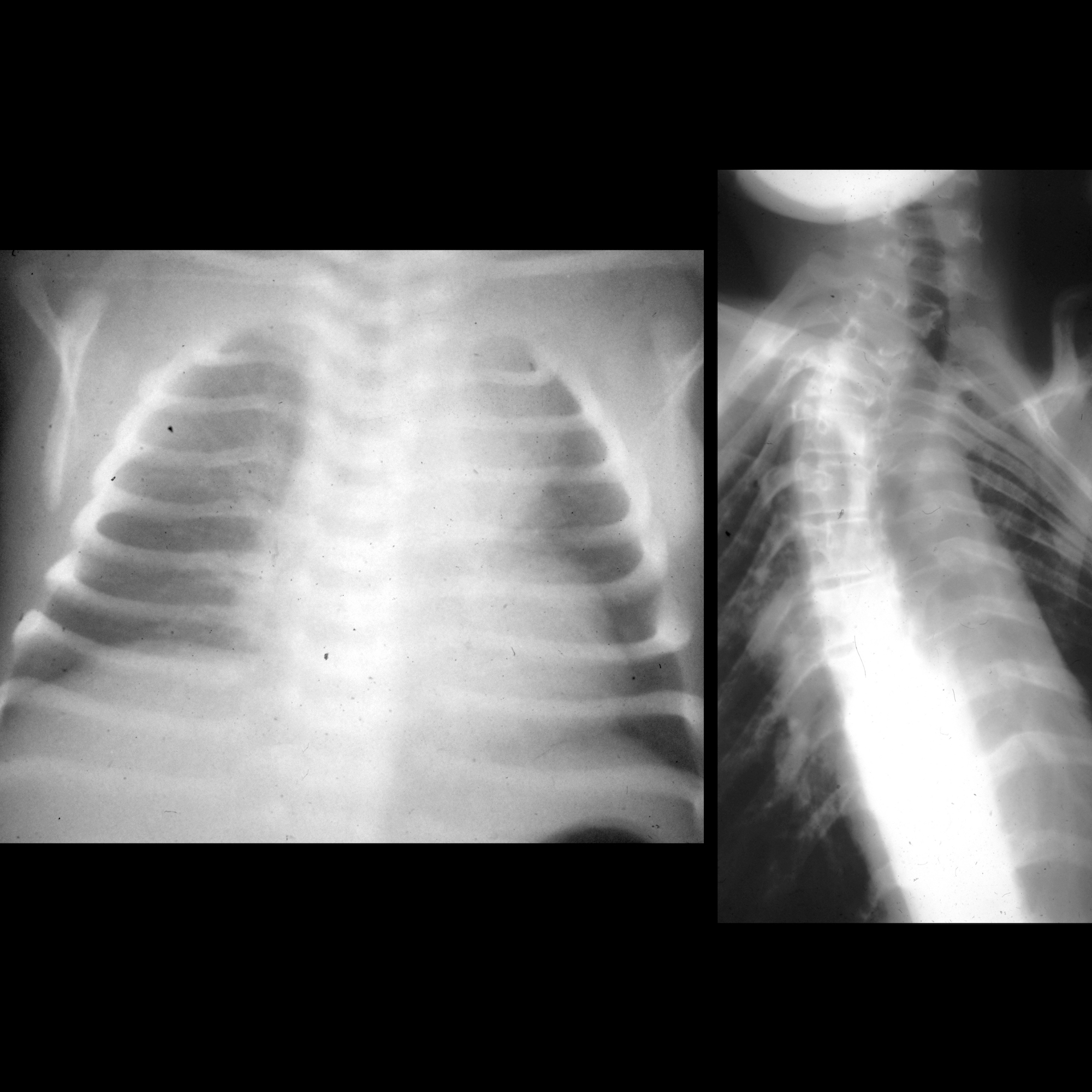











Scoliosis is defined as an abnormal lateral curvature of the spine. It is quite common in young individuals and is often idiopathic and asymptomatic. In some cases, however, it is the result of underlying structural or neurological abnormalities.
Terminology
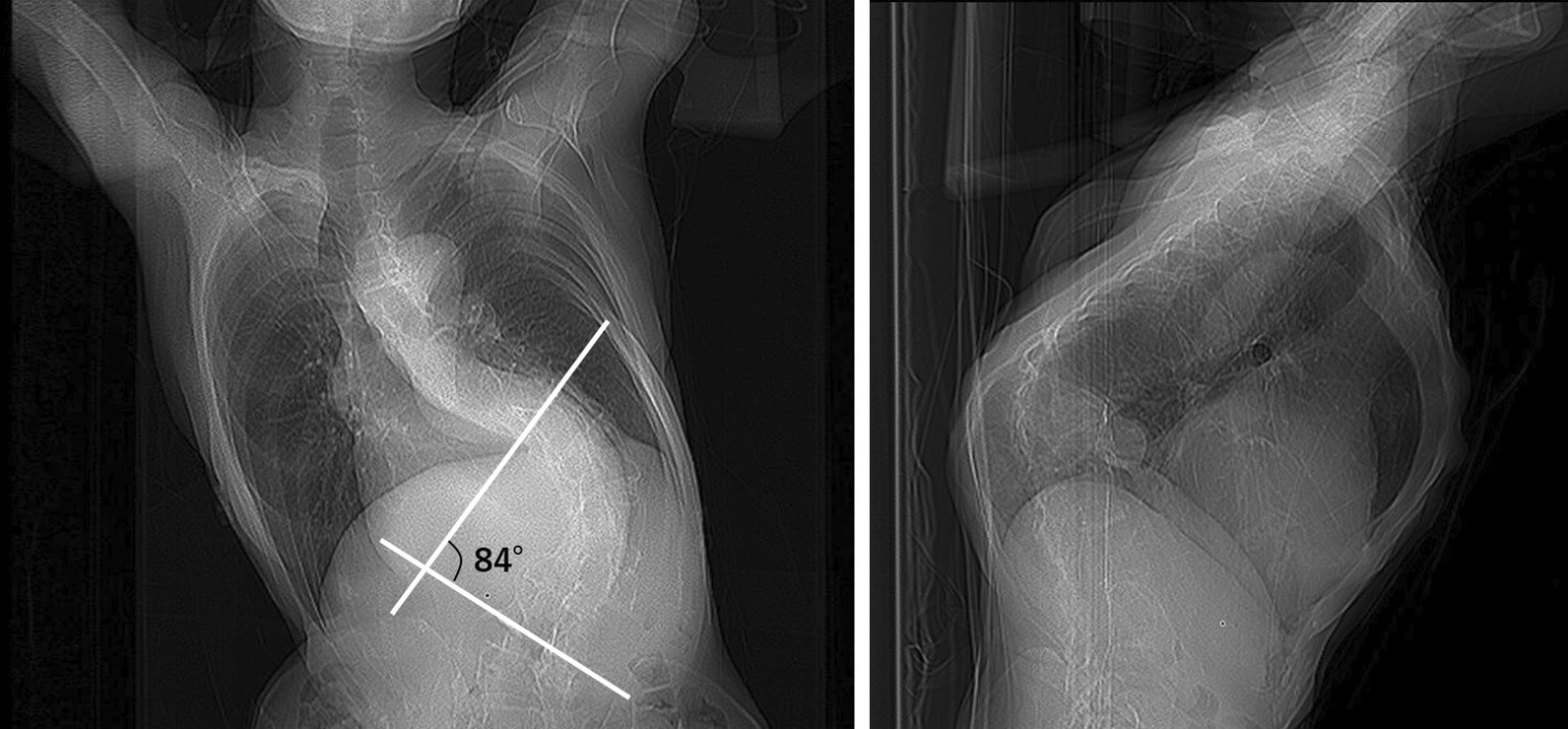
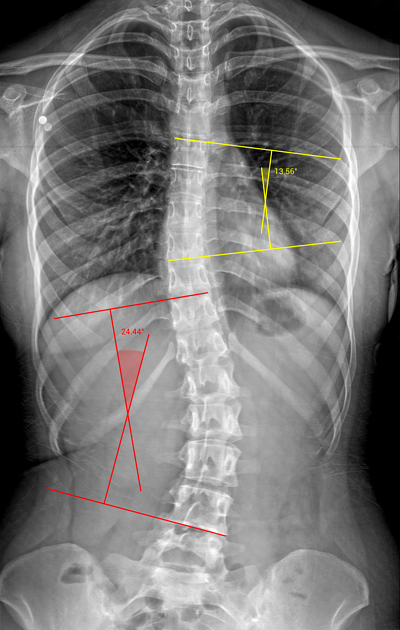
By definition, scoliosis is any lateral spinal curvature with a Cobb angle >10° with terms including:
- levoscolisois: curvature towards the left
- dextroscoliosis: curvature towards the right
Asymptomatic lateral curvature of the spine that is stable, with a Cobb angle ≤10° is known as spinal asymmetry
Clinical presentation
In most instances, scoliosis is obvious if severe. On examination, the Adams forward bend test (a clinical test for assessing scoliosis) may be positive where a rib hump forms on the side of the convexity.
Pathology
The majority (80%) of scolioses have no apparent underlying cause and are termed idiopathic . Scoliosis can also be broadly divided into being postural or structural.
Postural
Postural or non-structural curves are flexible, that is they correct with lateral flexion towards the convexity of scoliosis, and are not associated with segmentation abnormalities, rotational deformity, or vertebral body wedging. Postural curves may become secondarily fixed over time, when osseous changes, ligamentous shortening, and muscle atrophy occur.
Structural
Structural curves are fixed and are the result of a wide variety of causes:
- congenital scoliosis
- segmentation abnormalities (e.g. hemivertebrae)
- connective tissue disorders (e.g. Marfan disease)
- neurofibromatosis type 1
- skeletal dysplasias (e.g. achondroplasia)
- neuromuscular scoliosis
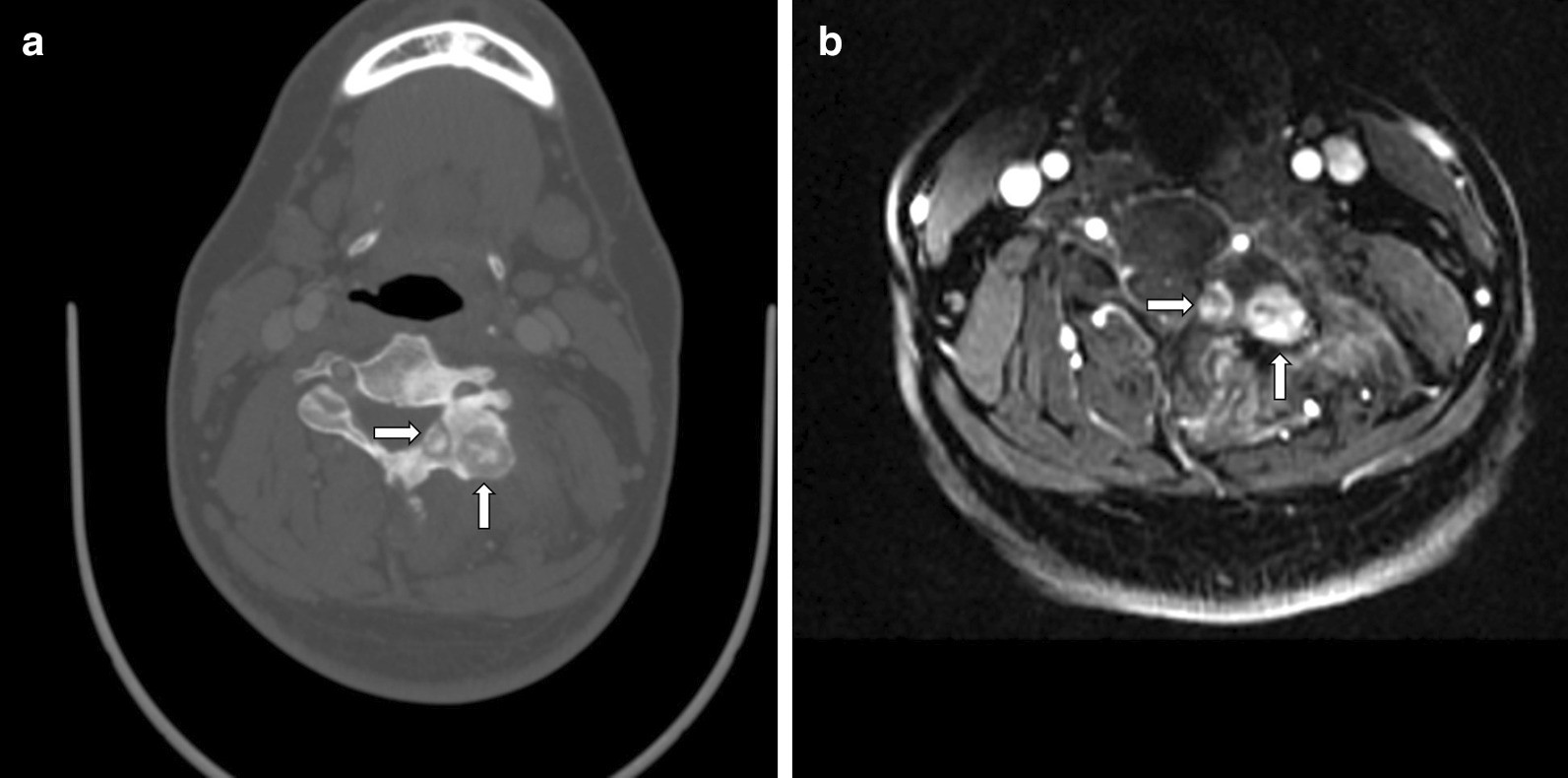
- infection resulting in bony abnormalities (e.g. pyogenic osteomyelitis, tuberculous spondylitis)
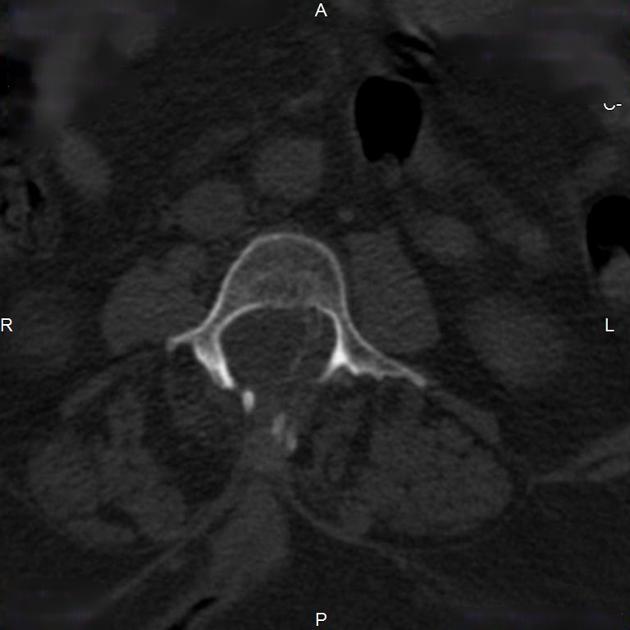
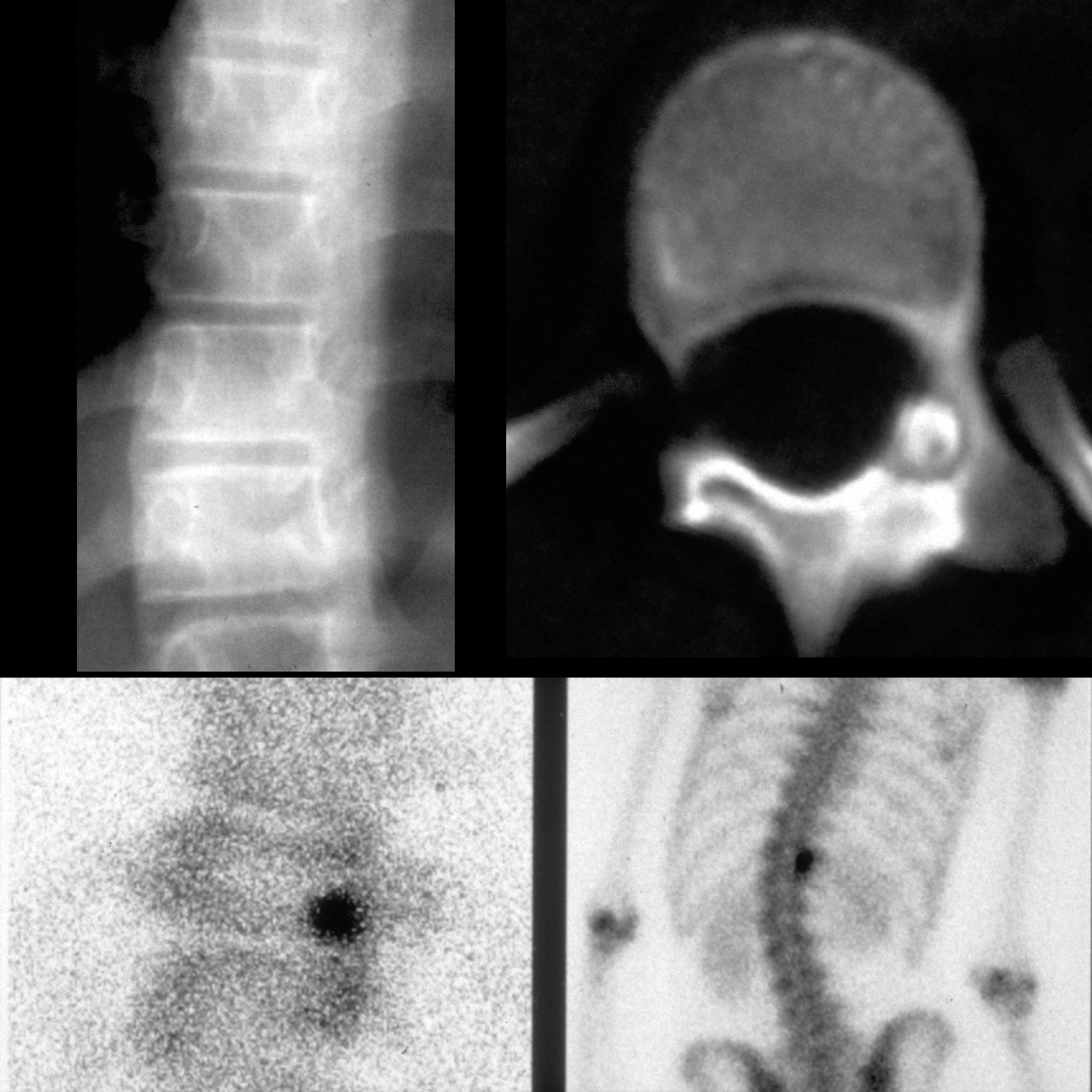
- tumors
- of bone: osteoid osteoma, osteoblastoma, metastases
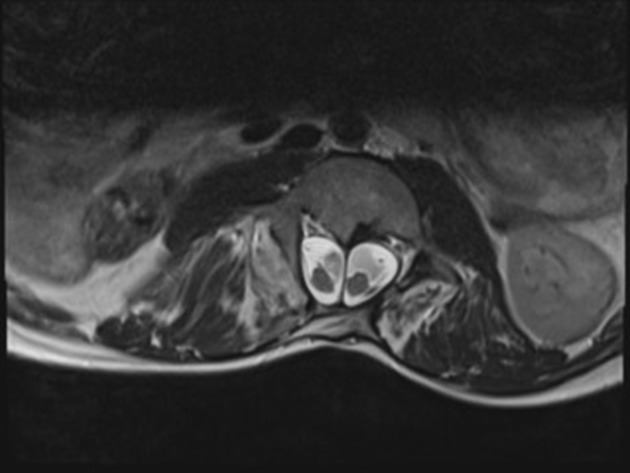
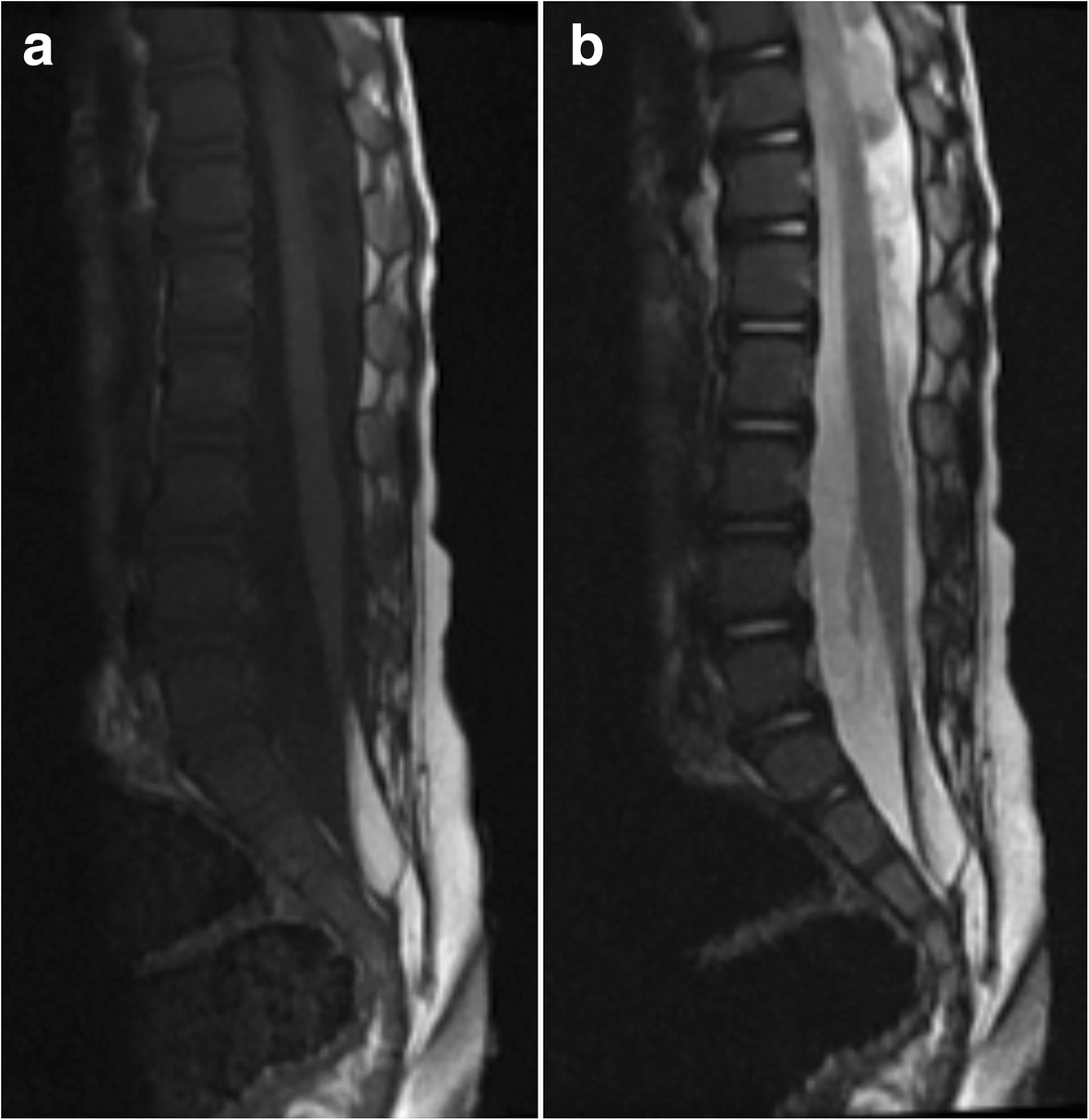
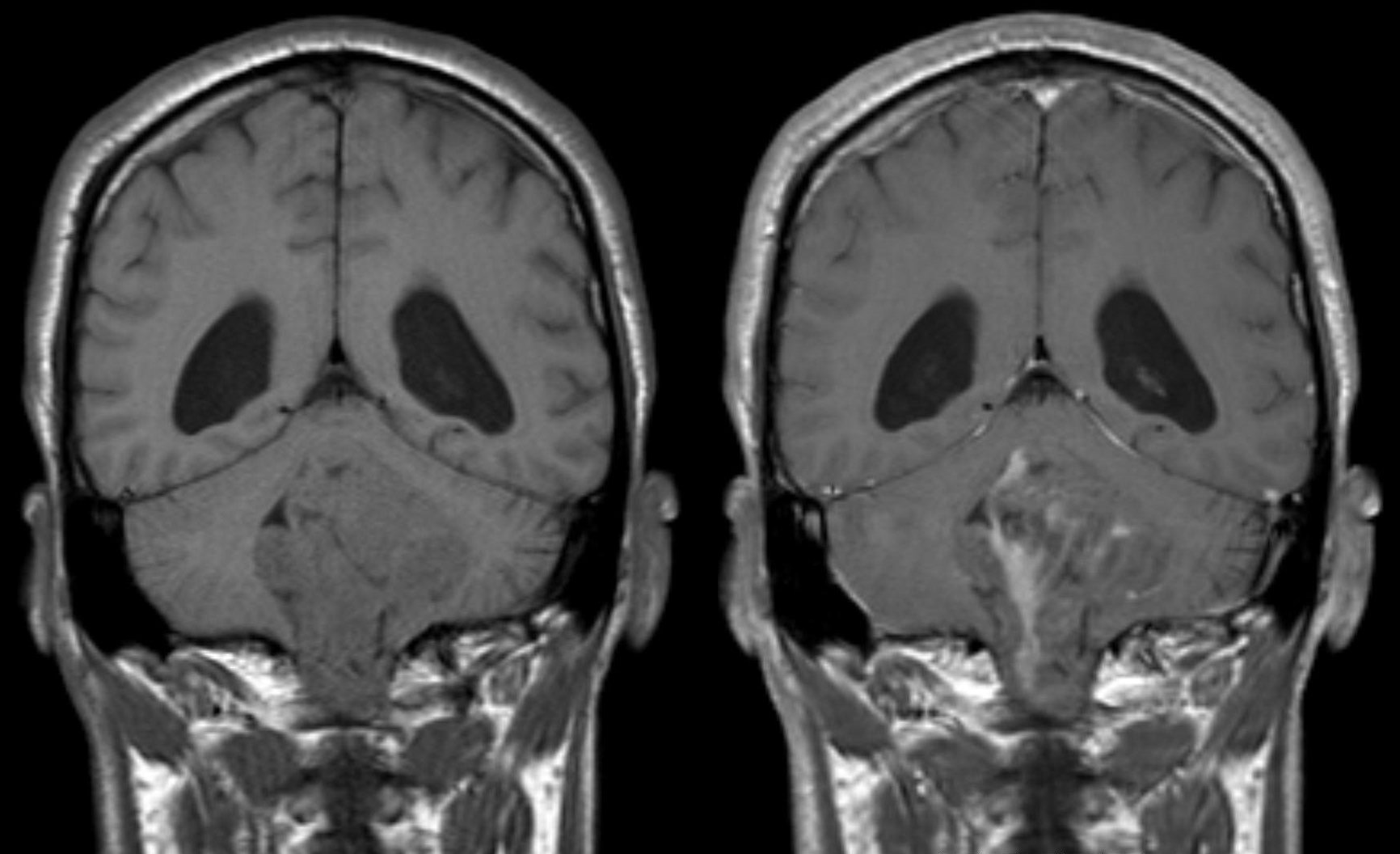
- of soft tissues: meningioma, neurofibroma, astrocytoma, ependymoma
Radiographic features
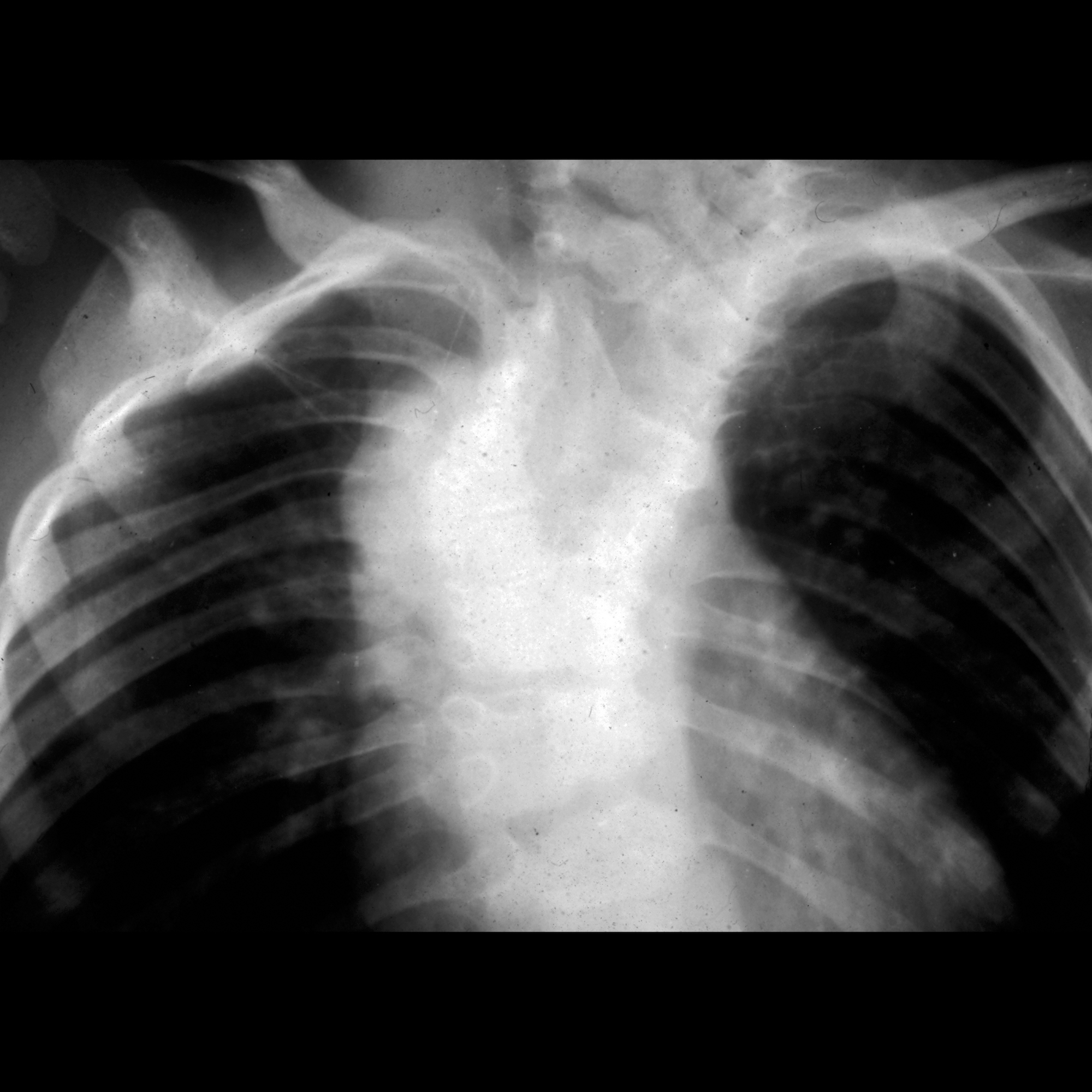
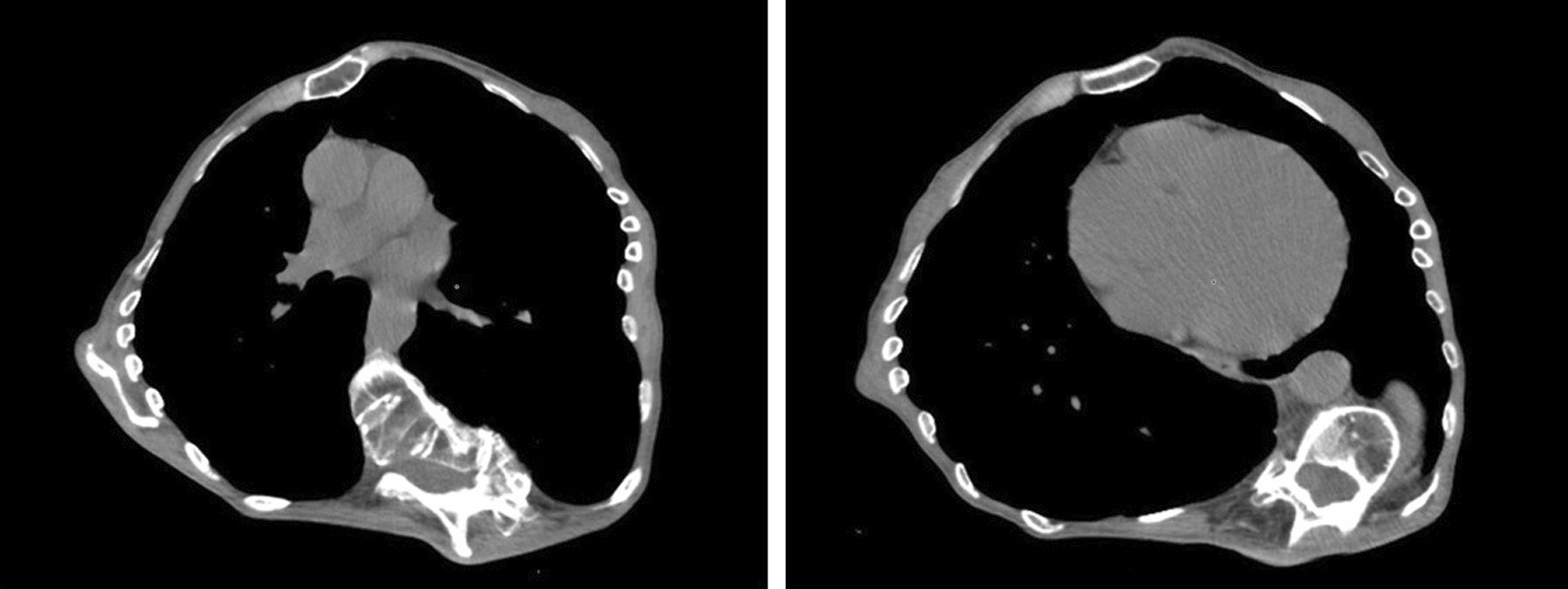
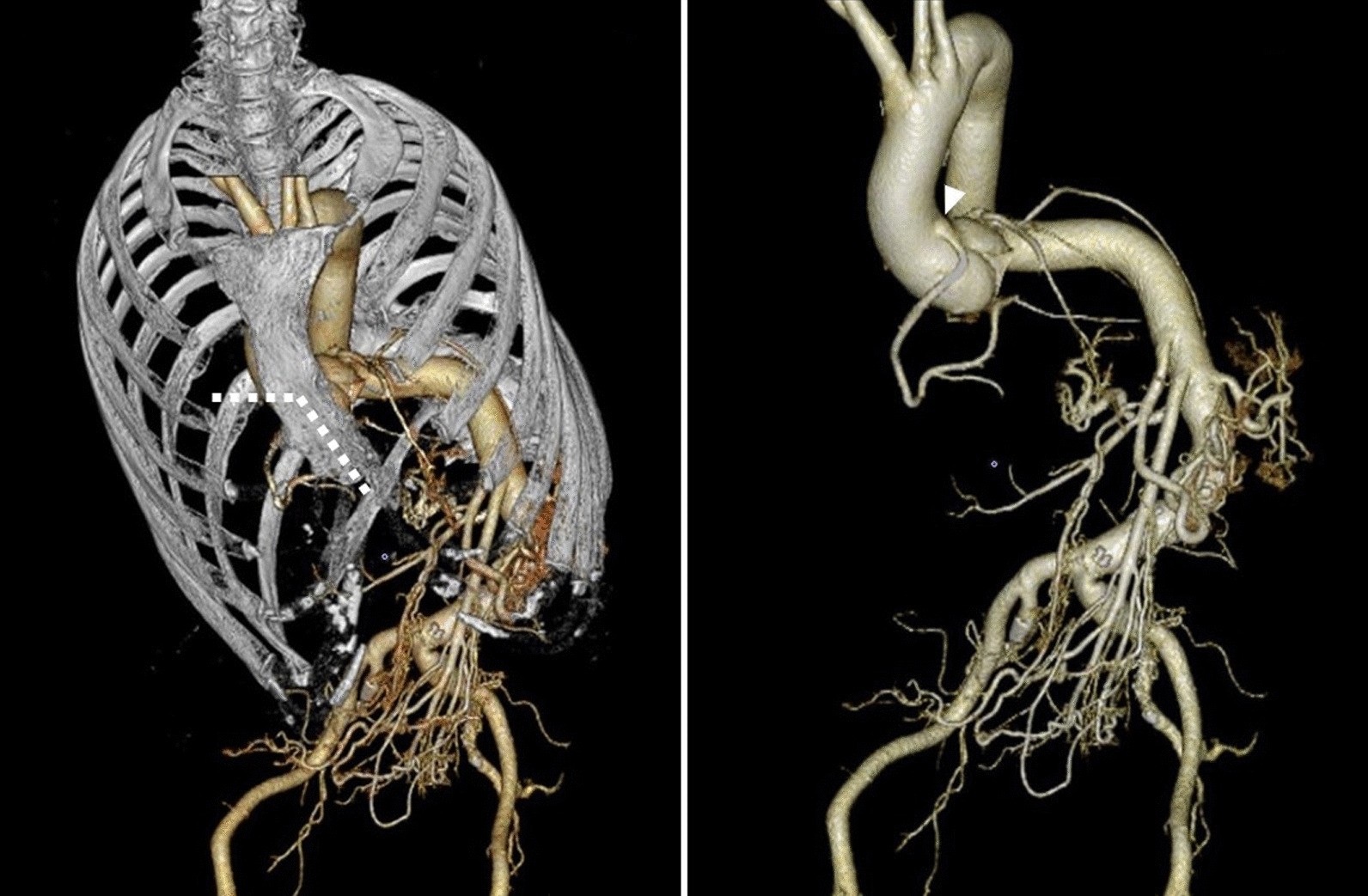
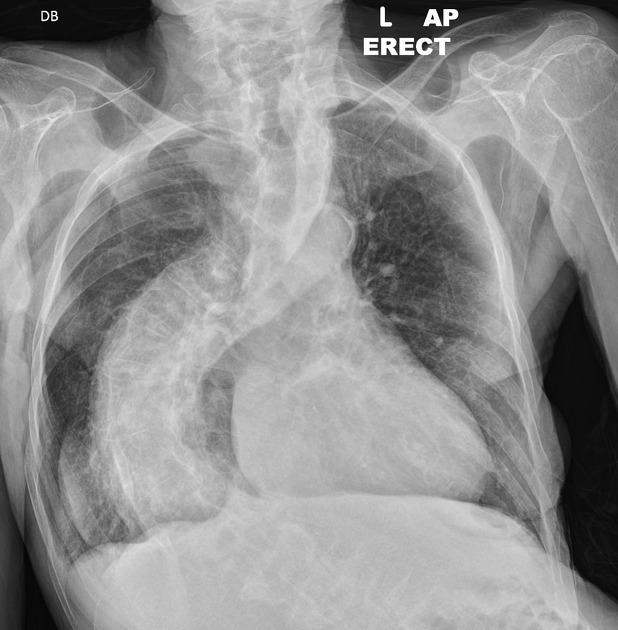
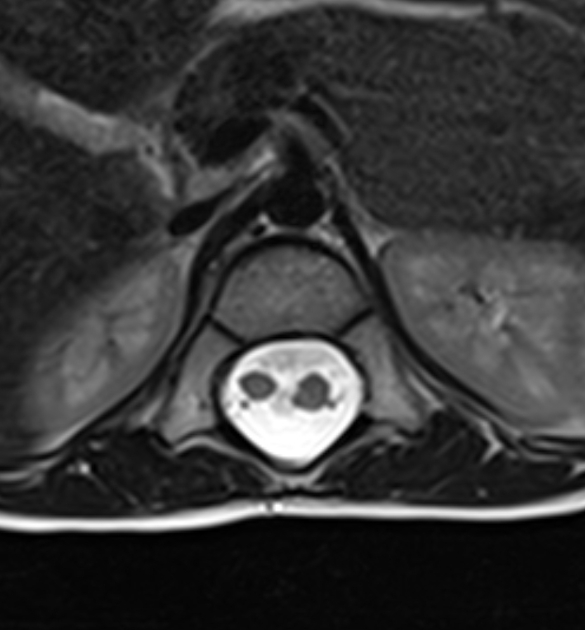
Assessment and monitoring of scolioses is primarily achieved with long-spine plain films in the PA and lateral projections. CT and MRI have roles to play in assessing for underlying abnormalities as well as, in certain situations, preoperative planning.
Plain radiograph
By convention scoliosis radiographs are displaced laterally flipped to all other imaging (left of the patient is on the left of the image), to replicate what the clinician views when standing behind the patient who is facing away.
Examination of spinal films should be systematic, and the following features should be assessed and commented upon :
- presence of structural osseous abnormalities
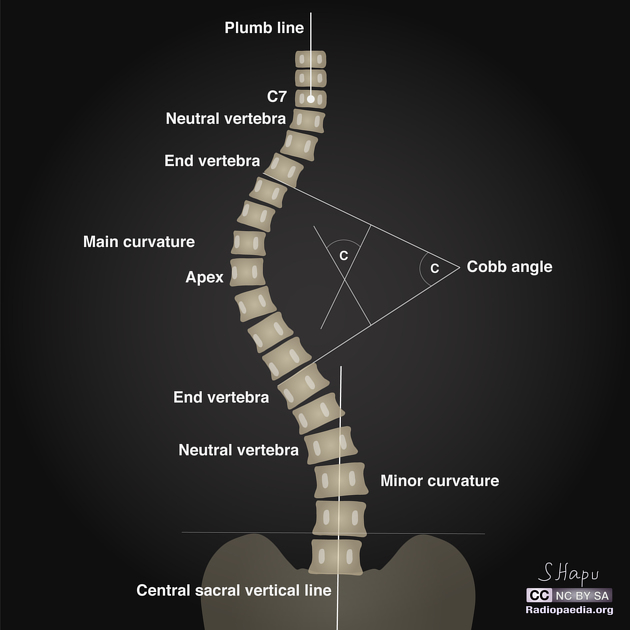
- major and minor curves
- apex
- end vertebrae
- neutral vertebrae
- stable vertebra
- sagittal and coronal balance
Major and minor curves
The major curve is the curve which is most pronounced and usually develops first . The major curve will usually have structural abnormality if such an abnormality is present.
Minor curves are compensatory curves, the result of trying to maintain balance in spite of the major curve. They are less pronounced and develop later than the major curve . They may be fixed or flexible.
Structural osseous abnormalities
The presence of vertebral body wedging, segmentation abnormalities (such as hemivertebrae), spina bifida, or destructive lesions should be sought.
Apex
The apex is the vertebral body or disc space which demonstrates the greatest rotation and/or furthest deviation from the expected center of the vertebral column . The endplates of the apical vertebra are often horizontal or near horizontal.
End vertebrae
The end vertebrae are present on either side of the apex and are the vertebrae which are most tilted towards each other . They form the basis of the Cobb angle.
Neutral vertebrae
Neutral vertebrae are present on either side of the apex and are the vertebrae which demonstrate no rotation (axial plane). In some cases, they will be the same as the end vertebrae although usually, they will be few segments more distal to the apex. They are never closer to the apex than the end vertebrae .
Stable vertebra
The stable vertebra is the first vertebra below the lowest curve which is roughly bisected by the central sacral vertical line (CSVL).
Sagittal and coronal balance
Sagittal balance and coronal balance refer to the overall alignment of the C7 vertebra with respect to the S1 vertebra. They require standing full spine films for assessment.
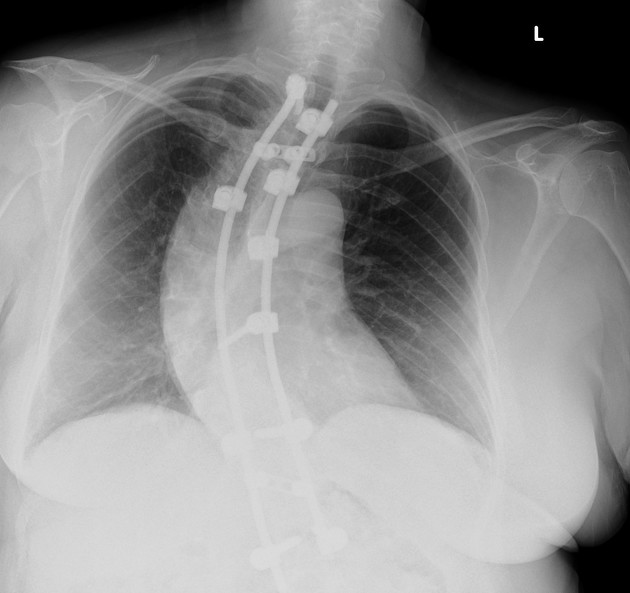
Treatment and prognosis
Management depends on the Cobb angle. At mild angles, observation or bracing may be considered, however for patients with a Cobb angle of ≥50° surgical intervention is often necessary .
Siehe auch:
- Tuberkulose
- Osteomyelitis
- Blockwirbel
- Osteoid-Osteom
- Ependymom
- Neurofibromatose Typ 1
- Astrozytom
- Neurofibrom
- Marfan-Syndrom
- Osteoblastom
- Skelettdysplasie
- Syringomyelie
- Tethered cord
- Proteus-Syndrom
- Diastematomyelie
- Halbwirbel
- Harrington-Stab
- Kongenitale Skoliose
- Spinale Muskelatrophie
- Harrington scoliosis
- Ichthyosis hystrix
- Cobb-Winkel
- schmerzhafte Skoliose
- adoleszente idiopathische Skoliose
- Dysrhaphie
- vertical expandable prosthetic titanium rib (VEPTR)
- hemivertebra with congenital scoliosis
- Skoliose nach Bestrahlung
und weiter:
- einseitig vermehrte Transparenz Thorax
- Klippel-Feil-Syndrom
- Tuberöse Sklerose
- cyllosoma
- Pectus carinatum
- kongenitale Radiusköpfchenluxation
- Turner-Syndrom
- Aicardi-Goutières-Syndrom
- Morbus Scheuermann
- Duraektasie
- Noonan-Syndrom
- dural ectasia of lumbo-sacral spine
- Rubinstein-Taybi-Syndrom
- MLO view
- Coffin-Lowry-Syndrom
- Spondyloepimetaphysäre Dysplasie Typ Strudwick
- Prader-Willi-Syndrom
- lumbosakrale Wirbelsäule bei Marfon-Syndrom
- Skelettreife nach Risser
- idiopathic scoliosis
- Kyphoskoliose
- radiologisches muskuloskelettales Curriculum
- VEPTR
- neuromuskuläre Skoliose
- Brustwanddeformitäten


 Assoziationen und Differentialdiagnosen zu Skoliose:
Assoziationen und Differentialdiagnosen zu Skoliose: