variant hepatic arterial anatomy
Variation in hepatic arterial anatomy is seen in 40-45% of people. Classic branching of the common hepatic artery from the celiac artery, and the proper hepatic artery into right and left hepatic arteries to supply the entire liver, is seen in 55-60% of the population.
Terminology
An accessory hepatic artery is one which arises from an anomalous origin and supplies a portion of the liver along with another artery.
A replaced hepatic artery is one which arises from an anomalous origin and supplies a portion of the liver solely.
Variant anatomy
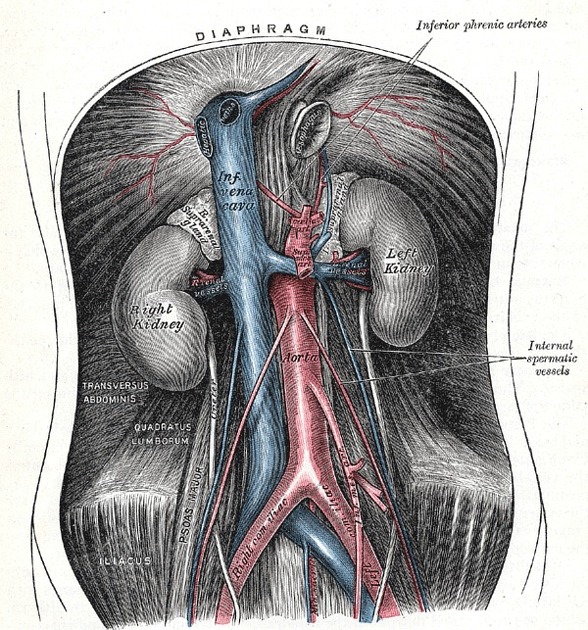
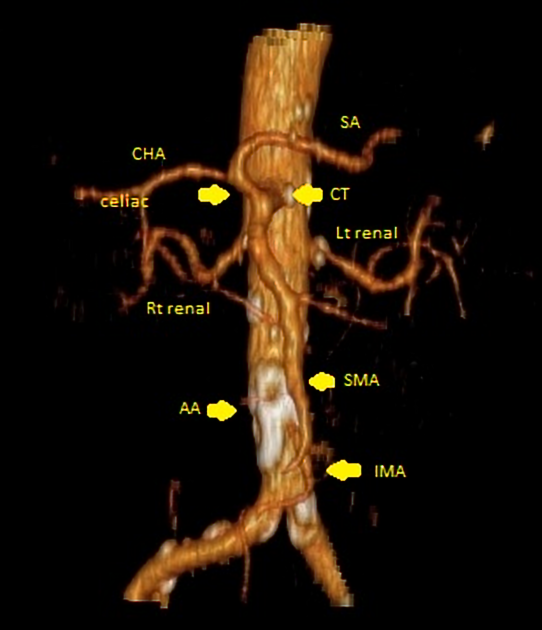
In general, the common hepatic artery may arise from the abdominal aorta or superior mesenteric artery (SMA) and all or part of the right and left hepatic arteries may arise from (be replaced to) other vessels.
The two most common variants are:
- replaced right hepatic artery arising from the SMA
- replaced left hepatic artery arising from the left gastric artery
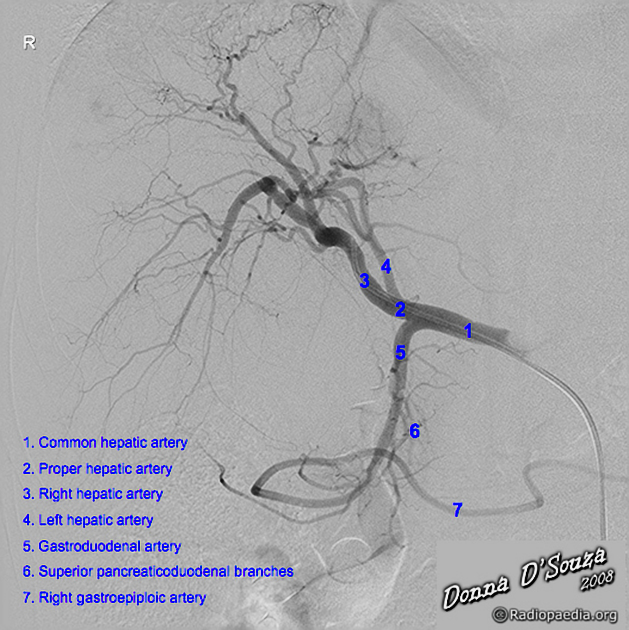
Another common finding, though not considered a variant by many authors, is trifurcation of the common hepatic artery into the right hepatic artery, left hepatic artery and gastroduodenal artery (GDA). With this branching pattern, there is no proper hepatic artery (PHA).
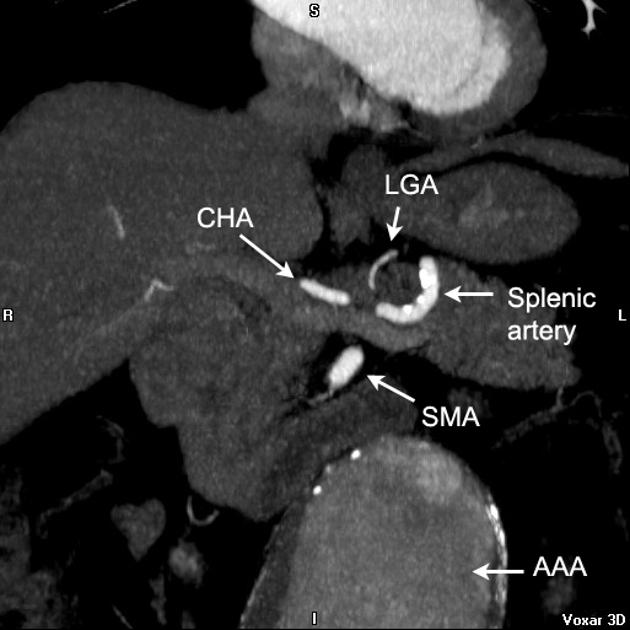
Common hepatic artery (CHA)
- from aorta: 2%
- from SMA: 2%
- trifurcation into RHA, LHA and GDA: ~6% (range 4-8%)
- from celiacomesenteric trunk (CMT)
Right hepatic artery (RHA)
- from celiac artery: ~2.5% (range 1-4%)
- from SMA: ~12.5% (range 9-15%)
- accessory right hepatic artery from SMA: ~4% (range 1-7%)
Left hepatic artery (LHA)
- from left gastric artery (LGA): ~7.5% (range 4-11%)
- accessory left hepatic artery from LGA: ~7.5% (range 4-11%)
Right and left hepatic arteries
- RHA from SMA and LHA from LGA: ~1% (range 0.5-2%)
- accessory RHA and LHA: 1%
Middle hepatic artery (MHA)
- middle hepatic artery usually arises from the left hepatic artery
- it may arise from the right hepatic artery
- it may arise as a trifurcation of the proper hepatic artery in the porta hepatis
- in patients with a replaced left hepatic artery, the middle hepatic artery arises from the right hepatic artery
- in patients with a replaced right hepatic artery, the middle hepatic artery arises from the left hepatic artery
- if the bifurcation of the proper hepatic artery is low within the porta hepatic, then the middle hepatic artery may have an extrahepatic course and traverse Calot's triangle
Classification
A classification method was described by Michel et al. in 1955
- I: standard anatomy ~60% (range 55-61%)
- II: replaced LHA ~7.5% (range 3-10%)
- III: replaced RHA ~10% (range 8-11 %)
- IV: replaced RHA and LHA ~1%
- V: accessory LHA from LGA ~10% (range 8-11%)
- VI: accessory RHA from SMA ~5% (range 1.5-7%)
- VII: accessory RHA and LHA ~1%
- VIII: accessory RHA and LHA and replaced LHA or RHA ~2.5%
- IX: CHA replaced to SMA ~3% (range 2-4.5%)
- X: CHA replaced to LGA ~0.5%
- unclassified
- CHA separate origin from aorta ~2%
- double hepatic artery ~4%
- PHA replaced to SMA; GDA origin from aorta <0.5%
See also
- variant hepatic venous anatomy
- anatomic variants
Siehe auch:
- Truncus coeliacus Varianten
- Aorta abdominalis
- Truncus coeliacus
- superior mesenteric artery (SMA)
- Arteria hepatica communis
- Varianten der Arteria mesenterica superior
- Arteria gastrica sinistra
- Chemoembolisation Komplikationen
- Arteria falciforme
und weiter:


 Assoziationen und Differentialdiagnosen zu Varianten der arteriellen Leberversorgung:
Assoziationen und Differentialdiagnosen zu Varianten der arteriellen Leberversorgung: